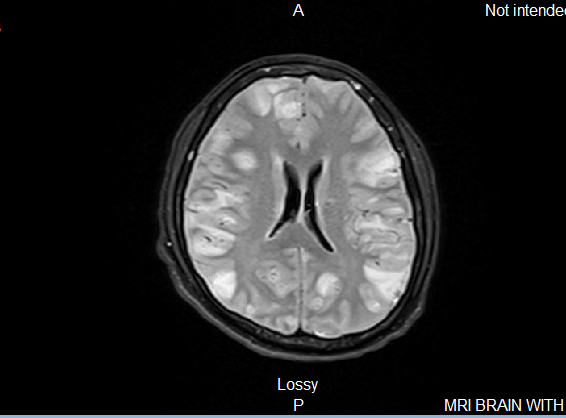
Case Presentation: We present a case of a 21-year-old previously healthy male with a history of marijuana use who was admitted to the hospital with neuropsychiatric symptoms, including confusion, agitation, disorganized behavior, and significant unintentional weight loss. The patient had recently moved to the United States from Guatemala. Initial examination revealed that he was disoriented and non-conversant, but without any focal neurological deficits. Other systems examination was largely unremarkable. Initial imaging showed multifocal ring-enhancing lesions concerning for neurocysticercosis versus CNS tuberculosis. A lumbar puncture showed lymphocytic pleocytosis with a bloody tap. The patient was started on empiric antimicrobial and antihelminthic therapy (praziquantel, steroids, and supportive agents). Despite appropriate therapy, his neurological status declined. He was transferred to a higher level of care for neurosurgical evaluation and critical care management and was eventually intubated. Neurosurgery placed an external ventricular drain (EVD) for management of severely elevated ICPs (sustained >70 mmHg) and obtained a tissue sample for biopsy. Repeat CSF analysis showed turbid fluid with markedly elevated RBCs and glucose. EEG demonstrated severe encephalopathy with electrographic seizures. The infectious disease team broadened antimicrobial coverage to include RIPE therapy for empiric treatment of CNS TB. Despite these interventions, including hyperosmolar therapy and initiation of pressors for hemodynamic support, the patient’s neurological status did not improve. The family opted for comfort measures, and the patient eventually succumbed to the disease after nine days of hospitalization.
Discussion: Neurocysticercosis is a CNS (Central Nervous System) infection caused by the larval form of Taenia solium (1). It is the most common parasitic disease of the CNS and the leading cause of acquired epilepsy worldwide (1). In humans, who are the intermediate hosts for the larval form of the Taenia solium tapeworm, cysticercosis is usually caused by ingestion of the parasite’s eggs via the fecal-oral route from other human carriers (2), and not by ingestion of contaminated undercooked pork, as is commonly believed. The CNS is commonly affected which may lead to a host of neurological symptoms—seizures being the most common (2). A large proportion of patients also develop focal deficits, increased intracranial pressure, and cognitive decline (2). Some severe cases of neurocysticercosis may prove fatal, as outlined in the case report.
Conclusions: The prevalence and mortality rates of neurocysticercosis is largely unknown in the United States due to the absence of effective surveillance (3,4). Although underreported, it is important to consider neurocysticercosis in the differential diagnosis during the initial assessment of a patient presenting with neurological or neuropsychiatric symptoms and typical imaging findings. Early diagnosis and prompt treatment can prevent the progression of neurological symptoms and, in some cases, may even prevent death (5). Early initiation of steroids in management may also help control inflammation associated with neurocysticercosis (6). There may be significant clinical benefit to pretreating with corticosteroids before administering anti-helminthic agents, which may trigger an acute immune response to the parasite (6). Thus, the use and timing of steroids in the management of neurocysticercosis are critical.