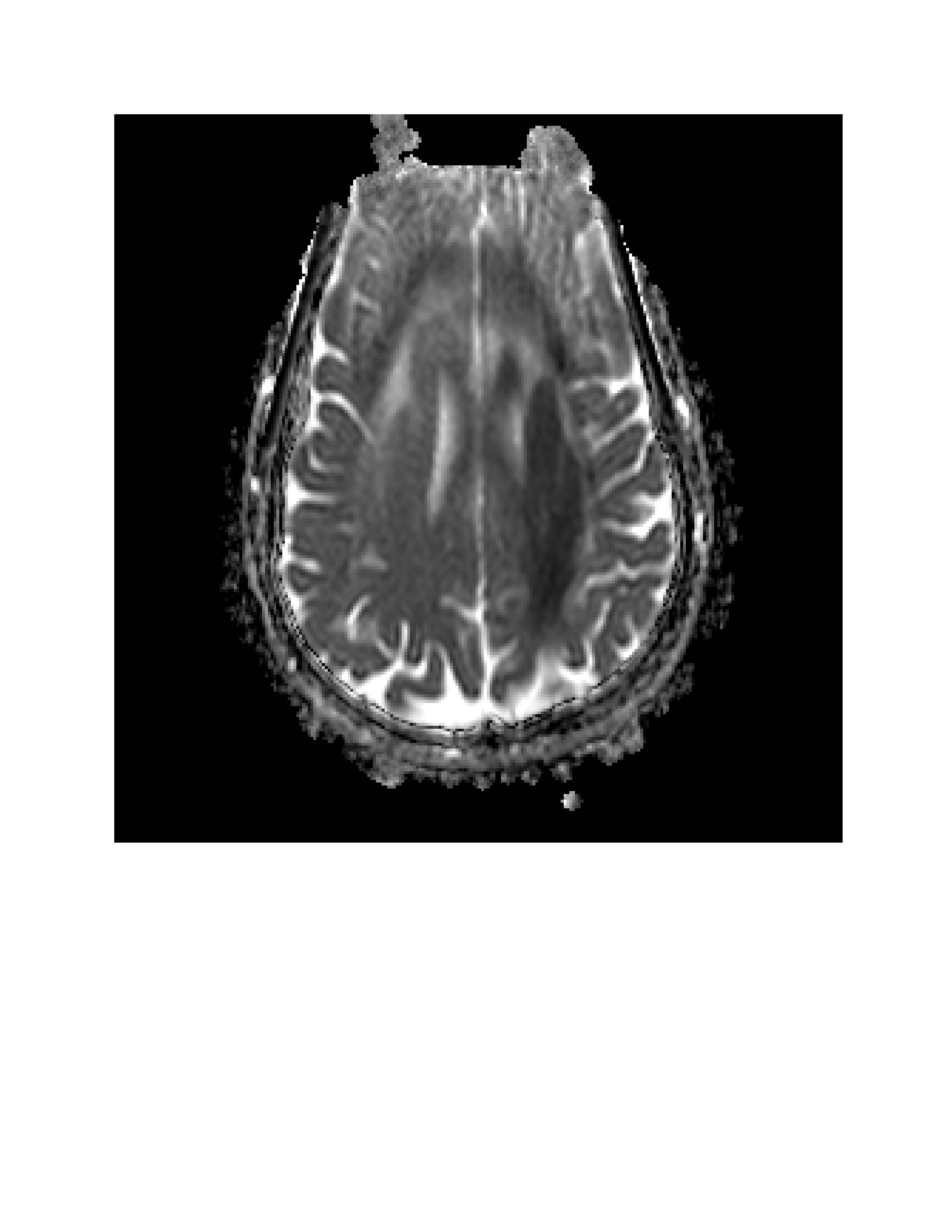
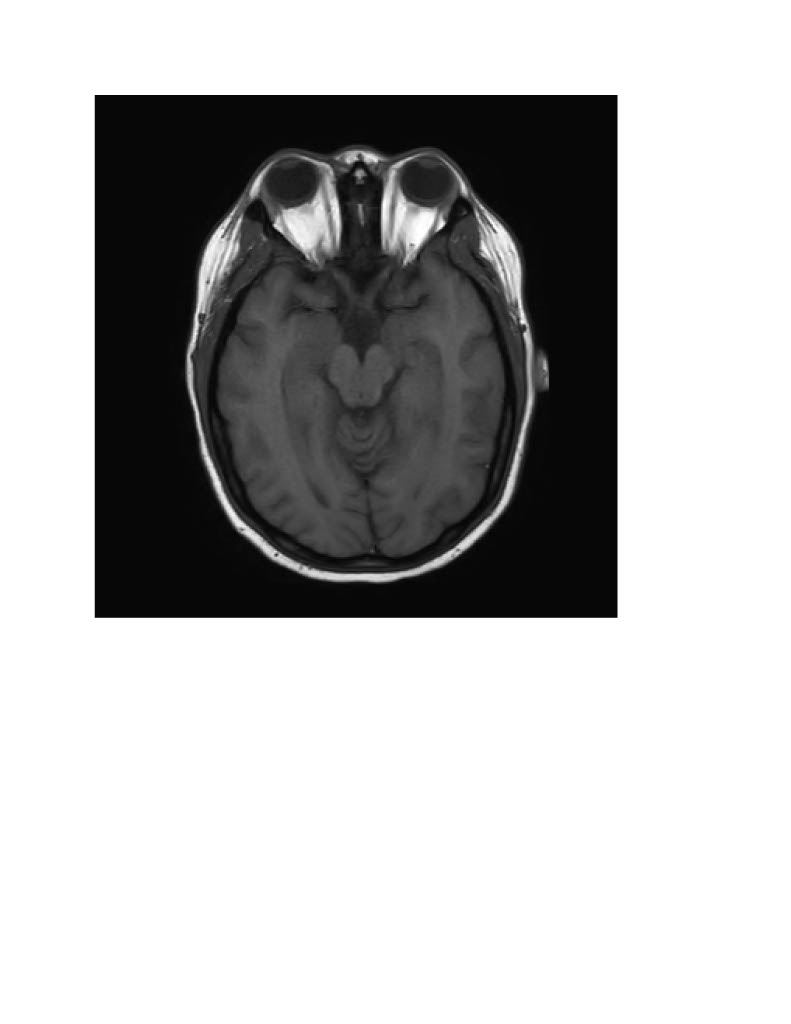
Case Presentation: A 21-year-old woman with no significant medical history presented to the hospital with altered mental status. Her mother, who was at the bedside, provided the clinical history. On arrival, the patient was nonverbal and exhibited right-sided hemiparesis and aphasia .Initial laboratory studies revealed leukocytosis, elevated inflammatory markers, transaminitis, and an elevated troponin level. She tested positive for COVID-19, while screening for hepatitis, HIV, and syphilis antibodies was negative. A urine drug screen was also negative. CT angiography of the head and neck was unremarkable, and cerebral perfusion imaging showed no abnormalities. However, brain MRI revealed abnormal signal changes predominantly in the left-sided white matter, with extension across the midline posteriorly through the corpus callosum. A right upper quadrant ultrasound showed fatty infiltration of the liver. Echocardiography was normal, and although cardiology considered a coronary CTA, it was deemed unnecessary on an emergent basis. MRI of the cervical and thoracic spine was unremarkable. EEG demonstrated mild to moderate diffuse cerebral dysfunction of nonspecific etiology. During hospitalization, the patient underwent a lumbar puncture, which yielded normal results. Her clinical presentation, combined with recent case reports, raised suspicion for COVID-19-related encephalitis. Neurology followed her case closely, and she was treated with a three-day course of intravenous Solu-Medrol (1 g). A follow-up brain MRI the next day showed resolution of the diffusion abnormality in the deep left cerebral white matter and thalamus. Given her significant clinical improvement, she was transitioned to dexamethasone (6 mg daily), which she completed over the following days. Her encephalopathy resolved, and her motor deficits improved substantially, allowing her to ambulate with a rolling walker. The patient was subsequently discharged with recommendations for follow-up with primary care, neurology, psychiatry, and physical therapy.
Discussion: This case underscores the importance of early recognition and timely immunomodulatory treatment in patients with COVID-19-associated neurological complications. A high index of suspicion for ADEM should be maintained in patients presenting with rapid-onset encephalopathy and focal neurological deficits, particularly in the context of a recent viral infection
Conclusions: As our understanding of post-viral immune-mediated neurological conditions continues to evolve, ongoing research is needed to refine diagnostic criteria and optimize treatment strategies for ADEM.