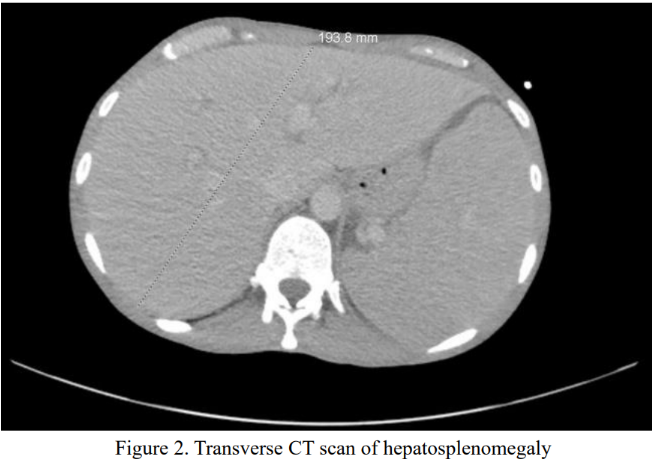
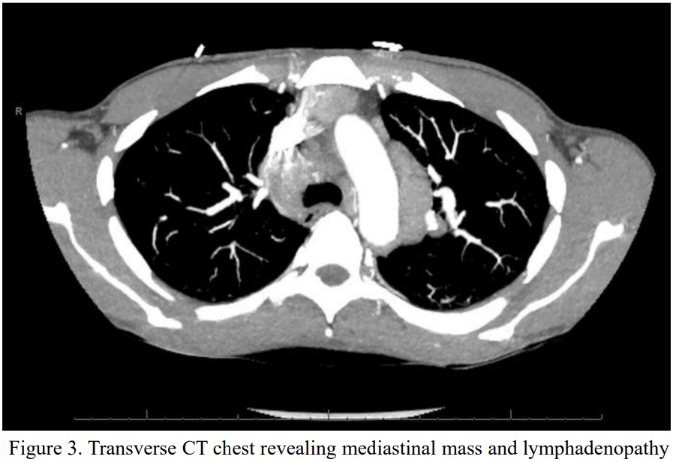
Case Presentation: A 42-year-old transgender female with recently diagnosed nodular sclerosing Hodgkin lymphoma presented after a syncopal episode in the setting of cachexia and malnutrition. She had been discharged the day prior after multiple transfusions and biopsy confirming Hodgkin lymphoma. On arrival, she was hypotensive, tachycardic, febrile, and hypoglycemic. She was diagnosed with distributive and hypovolemic shock, started on norepinephrine and broad antibiotics, and admitted to the intensive care unit. In the unit, she developed jaundice, thrombocytopenia, lactic acidosis, and rising oxygen needs, prompting mechanical ventilation. Paracentesis showed no spontaneous bacterial peritonitis. On day three, she had worsening hyperbilirubinemia and labs revealed ferritin 13,059 nanograms per milliliter, hemoglobin 8.7 grams per deciliter, platelet count 7,000 per microliter, fibrinogen 160 milligrams per deciliter, triglycerides 106 milligrams per deciliter. Computed tomography revealed splenomegaly. She was started on a chemotherapy regimen of doxorubicin, bleomycin, vinblastine, and dacarbazine. By day four, she developed anuric renal failure and was treated with plasmapheresis and continuous renal replacement therapy. She received 12 red blood cells, 3 plasma, and 6 cryoprecipitate transfusions. Despite aggressive care, her condition worsened, and she died. Post-mortem, interleukin-2 receptor alpha returned at 166,750 picograms per milliliter.
Discussion: Hemophagocytic lymphohistiocytosis is a rapidly progressive, often fatal hyperinflammatory syndrome triggered by uncontrolled immune activation, frequently secondary to hematologic cancers like Hodgkin lymphoma. Diagnosis relies on a combination of clinical and laboratory criteria, but not all are reliably present in critically ill patients. Our patient met four: fever, cytopenias, hyperferritinemia, and splenomegaly. Notably, she lacked hypertriglyceridemia, an expected marker, likely due to profound malnutrition. This atypical lab profile illustrates the diagnostic challenge in real-world hospital settings. Standard treatment includes high-dose corticosteroids and etoposide, along with therapy for the underlying malignancy. Our patient received steroids and chemotherapy but declined rapidly and etoposide was withheld due to clinical instability. Her outcome underscores a key hospital medicine dilemma: waiting for complete diagnostic criteria or confirmatory labs may delay life-saving treatment. In high-acuity cases with suggestive features, empiric therapy should be strongly considered. Early recognition and prompt intervention remain essential to improving survival, especially when presenting atypically.
Conclusions: Hemophagocytic lymphohistiocytosis should be considered in patients with malignancy, fever, and organ failure, as early recognition and treatment may improve survival even without full diagnostic criteria.