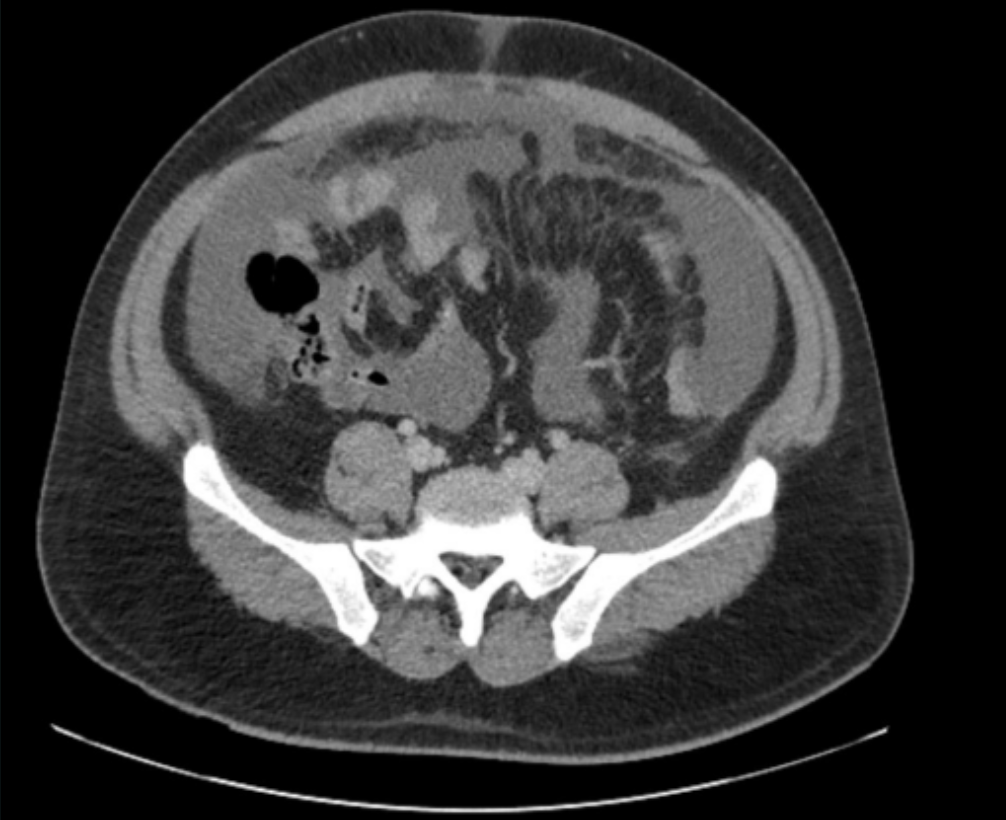
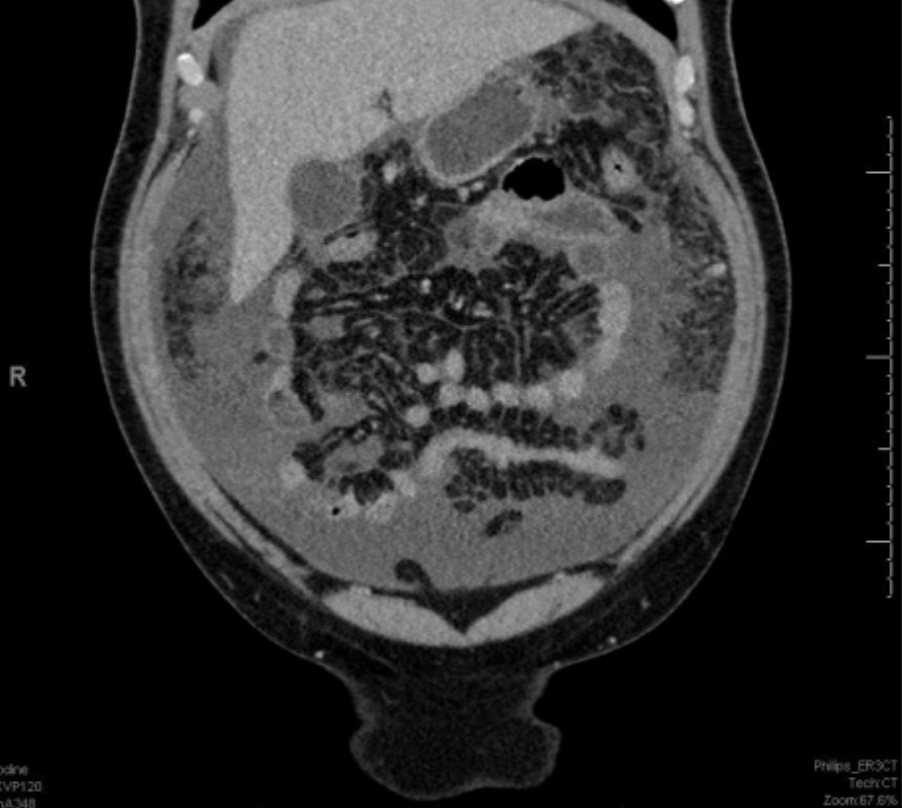
Case Presentation: Tuberculous peritonitis is a rare manifestation of extrapulmonary tuberculosis (TB) in the United States, accounting for approximately 6% of extrapulmonary cases and only a small fraction of total TB infections. We present a case of an immunocompetent young male whose acute abdomen with ascites initially suggested peritoneal carcinomatosis but was ultimately diagnosed as tuberculous peritonitis.A 32-year-old Hispanic male house painter with a history of weekend binge drinking presented with five days of progressive abdominal pain, distention, and subjective fevers. His occupational history included construction work in Guatemala and current employment with coworkers frequently traveling from Latin America. He reported worsening abdominal fullness and diffuse, tense pain unresponsive to NSAIDs, accompanied by two days of fevers, chills, and one episode of non-bloody emesis.He was hemodynamically stable. Laboratory evaluation showed mild leukocytosis (WBC 9.36 K/μL, neutrophils 76.5%), elevated AST (102 U/L), ALT (65 U/L), and hypoalbuminemia (2.96 g/dL). CT abdomen/pelvis revealed moderate ascites, peritoneal enhancement, omental thickening, and mildly enlarged pericardial lymph nodes—raising concern for peritoneal carcinomatosis versus infectious peritonitis.Abdominal Doppler ultrasound showed patent portal veins with hepatopetal flow, cirrhosis, and perihepatic ascites. Paracentesis revealed >250 polymorphonuclear cells/μL and lymphocytic predominance, prompting empiric antibiotics for presumed spontaneous bacterial peritonitis. Persistent fevers despite appropriate therapy led to further workup. Serum-ascites albumin gradient (SAAG) was < 1.1 g/dL, suggesting a non–portal hypertensive cause.Oncology consultation prompted gastroenterology (GI) evaluation, which in turn involved infectious disease (ID) due to concern for tuberculous peritonitis in the setting of exposure and imaging findings. QuantiFERON-TB Gold was positive on two occasions. Lymph node biopsy demonstrated non-caseating granulomas. Quadruple anti-tuberculous therapy (isoniazid, rifampin, pyrazinamide, ethambutol) was initiated, leading to marked clinical improvement. Sputum AFB stain was negative, but peritoneal fluid culture grew Mycobacterium tuberculosis after 29 days, confirming the diagnosis.
Discussion: This case emphasizes three pearls. First, tuberculous peritonitis remains a great mimicker—radiographic findings indistinguishable from carcinomatosis can misdirect evaluation toward oncologic workup, delaying definitive therapy. Second, occupational exposure history is paramount; workers in immigrant-heavy industries represent a high-risk population often overlooked in low-prevalence regions like Florida. Third, the atypical finding of non-caseating granulomas challenged diagnostic certainty, demonstrating that histopathology must be interpreted within epidemiologic and clinical context rather than as definitive exclusion criteria.
Conclusions: In the era of declining TB incidence, maintaining diagnostic vigilance for extrapulmonary manifestations prevents misdiagnosis as malignancy, avoids unnecessary invasive procedures, and enables life-saving antimycobacterial therapy. The absence of pulmonary symptoms should not deter consideration of TB in patients with appropriate exposures presenting with the presented imaging and laboratory findings.