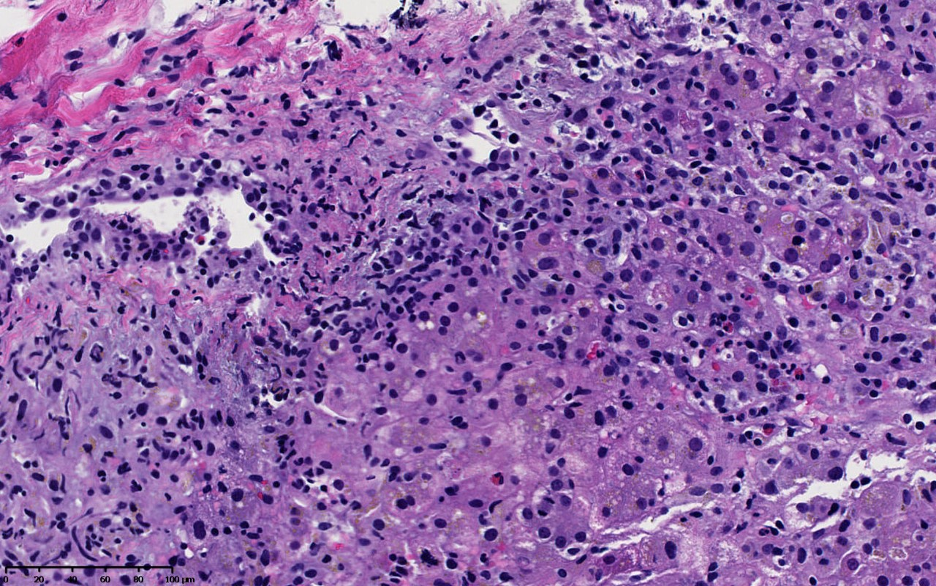
Case Presentation: A 22-year-old woman with macular lymphocytic arteritis presented to the hospital with a week of abdominal pain, vomiting, fatigue, and fevers. She had been initiated on dapsone one month prior for her arteritis, but stopped taking dapsone after her symptoms began. Prior to therapy, her Glucose-6-phosphate dehydrogenase (G6PD) activity was normal. On presentation, she was febrile to 39.4 degrees Celsius with pulse of 104 and blood pressure of 124/72. Examination revealed diffuse abdominal tenderness without rebound or guarding. Her mental status was intact. Her labs were notable for hemolytic anemia with a normal MCV, hemoglobin of 9.7, lactate dehydrogenase (LDH) 1492, haptoglobin < 31, and elevated reticulocytes at 3.3%. A Coomb’s test was negative. Her liver panel revealed hepatocellular and cholestatic patterns of liver injury, with an alkaline phosphatase of 168, AST (aspartate aminotransferase) of 611, ALT (alanine aminotransferase) 810, total bilirubin 4, direct bilirubin 2.68. Her International Normalized Ratio (INR) was 1.8. A right upper quadrant abdominal ultrasound showed gallbladder wall thickening. Despite negative infectious workup and empiric antibiotic therapy covering gram negative and anaerobic bacteria, she remained persistently febrile. A broad workup for causes of liver injury including viral and autoimmune hepatitis, Wilson’s disease, Alpha-1-antitrypsin deficiency, and hemochromatosis, was negative. Her liver enzymes and coagulopathy worsened and she was transferred to a liver transplant center and started on N-acetylcysteine infusion. At transfer, eosinophil count had increased to 15 from 0.6, and she had developed a non-pruritic rash on her bilateral upper extremities, scattered ill-defined erythematous round plaques without scaling or crust. Given the concern for DRESS syndrome (drug reaction with eosinophilia and systemic symptoms), specifically dapsone hypersensitivity syndrome (DHS), she underwent liver and skin biopsies which were consistent with DHS. She was started on prednisone, and her symptoms and labs began to improve. Her RUCAM (Roussel Uclaf Causality Assessment Method) score was calculated to be 8, suggesting probable causality.The liver biopsy was notable for severe acute necro-inflammatory injury with apoptotic bodies, diffuse sinusoidal lymphocytic infiltrate, and numerous eosinophils.
Discussion: Dapsone hypersensitivity syndrome (DHS) is a severe idiosyncratic reaction and variant of DRESS that occurs in 0.5 to 3.6% of patients treated with dapsone, characterized by fever, rash, eosinophilia, and systemic involvement.Hypersensitivity reactions to dapsone are associated with a fatality rate of approximately 10 percent. Symptoms of DHS typically arise within weeks of initiating dapsone, but can present as late as six months after its use. Symptoms most often include fever, severe fatigue, generalized cutaneous rash, and lymphadenopathy. Workup often reveals hemolytic anemia and hepatitis with mixed hepatocellular and cholestatic liver injury.The mechanism by which DHS occurs remains unclear, although there is evidence that variability in the production of reactive metabolites plays a role in sulfonamide hypersensitivity reactions.
Conclusions: Due to the rarity of DHS and the potentially fatal associated organ dysfunction, it is important to retain a high index of suspicion based on the medical history and clinical picture to make an early diagnosis, promptly withdraw dapsone, and administer glucocorticoids.