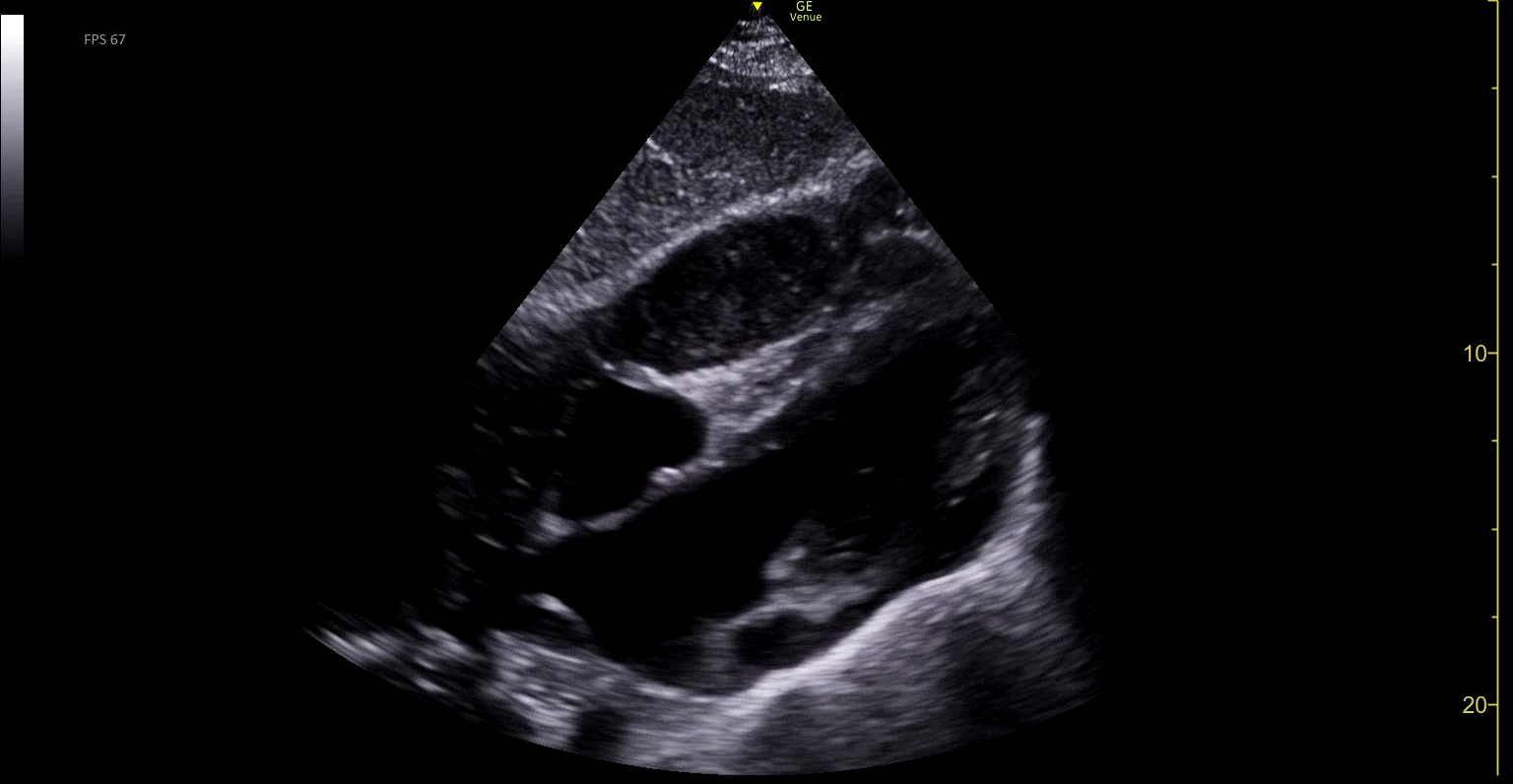
Case Presentation: A 46-year-old incarcerated patient with negligible past medical history experienced four months of right shoulder pain and later developed shortness of breath. His shoulder pain was evaluated by the prison’s medical staff. He was diagnosed with shoulder impingement. The patient suffered two syncopal events, which prompted hospital admission. Upon presentation, the patient had dyspnea on exertion and severe shoulder pain even at rest. Imaging revealed a right pleural effusion and a complex mediastinal mass compressing the right side of his heart. The pleural effusion was visible on standard POCUS lateral lung views. The mediastinal mass was best seen on a sub-xyphoid cardiac view and can be seen compressing the right ventricle. While the mediastinal mass was easily discernable to a team of hospitalists experienced in interpreting POCUS images, it could have easily been mistaken for a right ventricle with impaired filling. This more nuanced finding could be called “false ventricle sign.” The patient underwent chest tube placement for drainage of his hemothorax and CT-guided biopsy of the mass, which revealed synovial sarcoma. Surgical oncology determined that the mass size and distribution surrounding great vessels rendered the sarcoma unresectable. He discharged to the prison’s infirmary and transferred back to the hospital for initiation of chemotherapy. Pending his response to chemotherapy, he will be reevaluated for possible surgical resection of the tumor and radiation therapy.
Discussion: Point-of-Care Ultrasound (POCUS) can aid in risk stratification of dyspnea in outpatient settings, and in investigating atypical symptoms which may not otherwise prompt advanced imaging. In underserved areas, if obtaining diagnostic imaging is an obstacle, patients with lower pretest probability of cardiopulmonary pathology may not receive dedicated imaging. In this patient’s case of monthslong symptoms, POCUS could have expedited detection of his advanced malignancy. With the rise of POCUS availability, it will be particularly important to support underserved clinics in incorporating POCUS into their toolkit, to aid in rapid evaluation and early diagnosis of conditions visible on ultrasound.
Conclusions: ACP Guidelines recommend POCUS as part of a complete workup for dyspnea in emergency department and inpatient settings*. As POCUS becomes more widely available, its use in outpatient and particularly underserved settings could help improve patient outcomes. In the case of this incarcerated patient with four months of shoulder pain and dyspnea, syncope prompted hospital admission, where his POCUS lung exam revealed a large pleural effusion and cardiac mass. Had POCUS been available and part of a standard dyspnea workup in his outpatient setting, his pleural effusion would have prompted advanced imaging and presumably earlier detection of his malignancy. A standard POCUS cardiac exam also demonstrated a mass which mimicked the appearance of a poorly functioning right ventricle, in what could be called “false ventricle sign.” The honing of POCUS image acquisition and interpretation skills requires access to resources and support. This “false ventricle sign” required more nuance to interpret even amongst hospitalists in a setting where POCUS is readily available. As POCUS is more widely incorporated into outpatient practices, training and support of providers in underserved areas could lead to improved risk stratification and diagnosis of patients experiencing cardiopulmonary symptoms.