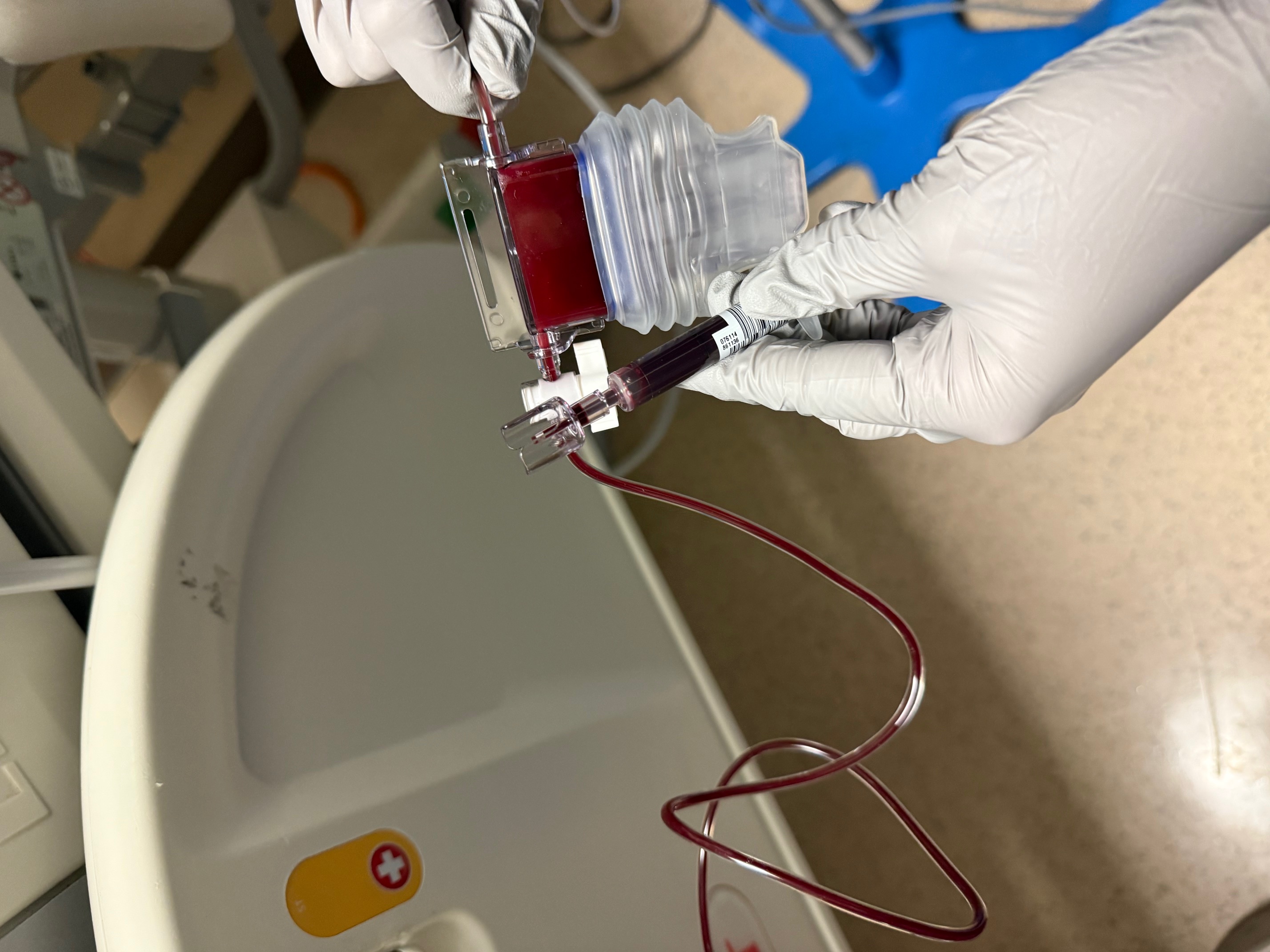
Case Presentation: A 95-year-old woman required admission for asymptomatic hypoxemia incidentally discovered at her nursing home with an oxygen saturation (SpO2) of 57% while breathing ambient air. The cardiopulmonary examination was unremarkable, and peripheral cyanosis and clubbing were absent. Chest imaging was normal. Her SpO2 failed to improve despite administration of 15L of oxygen via non-rebreather and subsequent bilevel positive pressure ventilation (BIPAP). Arterial blood gas analysis revealed a partial pressure of oxygen (PaO2) of 488 mmHg while on BIPAP with an FiO2 of 100% and subsequently a PaO2 of 67 mmHg while breathing ambient air; the blood was noted to be dark (Figure 1). The methemoglobin level was 2.6%. Other notable studies included a hemoglobin of 8.4 g/dL, an undetectable haptoglobin, an elevated lactate dehydrogenase, and moderate schistocytes on peripheral smear. Medication reconciliation revealed a one-month history of phenazopyridine use for urinary spasms, raising concern for both sulfhemoglobinemia and hemolytic anemia resulting from this medication. Phenazopyridine was discontinued, and two units of packed red blood cells (RBC) were transfused. The patient remained asymptomatic, and supplemental oxygen was weaned to target an acceptable PaO2. Following discharge, the sulfhemoglobin level resulted at 11% (upper limit of normal 2%), confirming the diagnosis of sulfhemoglobinemia.
Discussion: Sulfhemoglobinemia occurs when sulfur binds the porphyrin ring of hemoglobin and shifts the hemoglobin-dissociation curve to the right, assisting in tissue oxygenation [1]. It presents with falsely and dramatically low SpO2 readings due to altered wavelength absorption with pulse oximetry [1,2]. Many prescription and over-the-counter drugs are associated with the development of sulfhemoglobinemia by increasing levels of sulfur oxide in the blood, including phenazopyridine [3]. This drug is often used alongside antibiotics for the treatment of urinary tract infections to reduce urinary irritation, with use usually limited to two days [3]. Prolonged use or misuse of phenazopyridine can cause both sulfhemoglobinemia and hemolytic anemia. Diagnosis of sulfhemoglobinemia is challenging as most hospitals’ co-oximeters can detect other dyshemoglobins like methemoglobin or carboxyhemoglobin, however sulfhemoglobin often requires a send-out lab [4]. Suspicion of sulfhemoglobinemia should be considered if other dyshemoglobinemias have been ruled out. Treatment involves discontinuing the offending medication, supportive care, and RBC transfusion in the most serious cases.
Conclusions: Hypoxemia is a common reason for admission to the hospital. Hypoxemia refractory to supplemental oxygen requires an expanded differential diagnosis to include shunts and dyshemoglobinemias. Sulfhemoglobinemia is a rare dyshemoglobinemia that is not identified on routine blood gas analysis with co-oximetry. Careful review of medications can identify culprit drugs that should be discontinued.