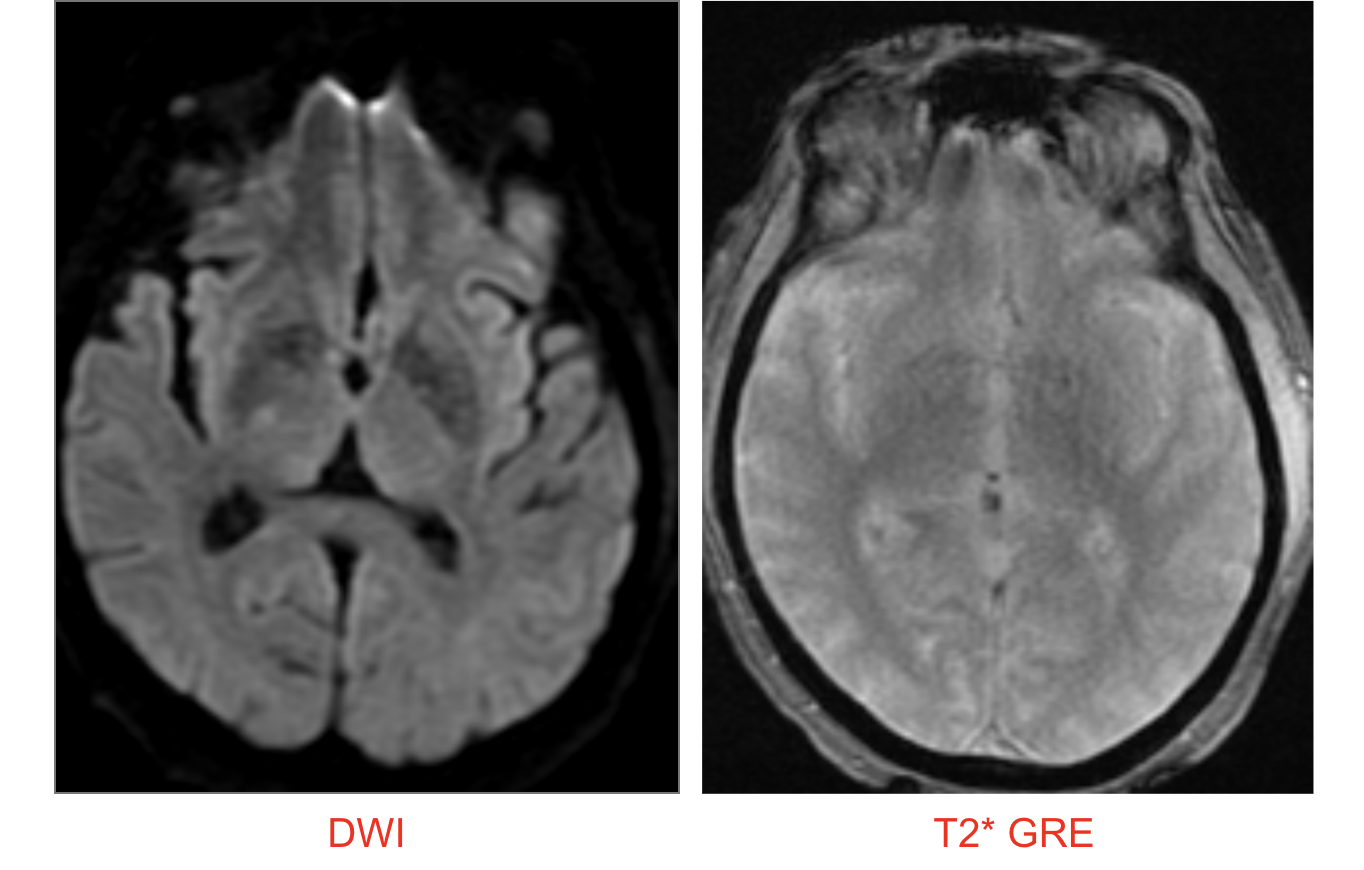
Case Presentation: A 61-year-old man with hypertension, hyperlipidemia, and a presumed diagnosis of Parkinson disease was admitted after sustaining burn injuries following a ground-level fall with loss of consciousness. CT head revealed a left extra-axial hypodensity with mild mass effect and bilateral basal ganglia hypodensities. One year earlier he developed a resting tremor of the left hand, followed by imbalance and recurrent falls. Six months before admission he was diagnosed with Parkinson disease by his primary physician, but never initiated therapy. After his most recent fall, he reported new sensory loss of the left face, arm, and leg.Neurologic examination showed decreased eye blink, hypokinetic dysarthria, left arm tremor, cogwheel rigidity (right > left), bilateral bradykinesia, increased tone in the legs, diminished sensation in the left hemiface and extremities, mild postural instability, freezing, retropulsion, and reduced arm swing. Carbidopa/levodopa was initiated. MRI brain demonstrated bilateral globus pallidus intrinsic T1 hyperintensity with associated T2/FLAIR signal. There was no associated diffusion signal abnormality or susceptibility on T2*GRE. Further history revealed that he had lived in a mobile home for six years, where he regularly melted manganese bronze, an alloy commonly used in jewelry-making, in his oven. He discontinued this practice 18 months earlier after losing the home.
Discussion: Manganese is an essential trace element with important enzymatic functions, yet chronic exposure can result in preferential basal ganglia deposition and progressive neurotoxicity. Occupational sources include smelting and welding, while in this case, repeated exposure to manganese bronze during jewelry-making in an enclosed living space was the likely cause.The clinical overlap with idiopathic Parkinson disease (resting tremor, bradykinesia, rigidity, masked facies) makes misdiagnosis common. However, rapid progression, early postural instability, and the characteristic MRI finding of bilateral globus pallidus signal abnormality, strongly suggest manganese toxicity.Management hinges on removal from exposure. Chelation with CaNa2EDTA can reduce systemic manganese levels but penetrates poorly into the CNS, limiting neurologic recovery. Levodopa therapy may provide partial relief, as observed with this patient’s tremor, but sustained benefit is uncommon, and progression often continues despite treatment. Early recognition and prevention remain the most effective strategies.
Conclusions: Manganese toxicity is a rare but clinically significant mimic of Parkinson disease. Careful attention to social and occupational history combined with targeted neuroimaging can uncover the diagnosis and prevent irreversible neurological decline. Recognition of atypical features in presumed Parkinson disease is essential to avoid misdiagnosis and guide appropriate management.
.png)