Background: Hospital readmissions have potent implications on patients and healthcare systems as they are frequently used as a surrogate for the quality of patient care. The Hospital Readmission Reduction Program was created to reduce Medicare reimbursement for hospitals with above expected 30-day readmission rates. As a result, many studies have evaluated themes among preventable readmissions that may represent targets for interventions to reduce readmission rates.
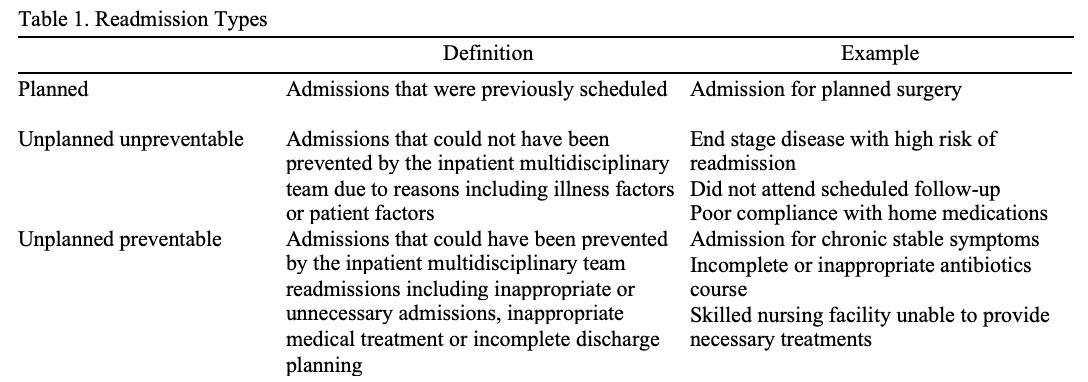
Purpose: We sought to better understand common readmission themes at our own institution by first examining the perspective of the discharging provider via the creation of a readmission survey where discharging providers were asked to classify 30-day readmissions as planned, preventable or unpreventable. We further investigated these 30-day readmissions by creating a readmissions committee consisting of hospitalist providers to analyze the survey data using agreed upon criteria (Table 1) to similarly adjudicate readmissions and evaluate agreement with the discharging providers.
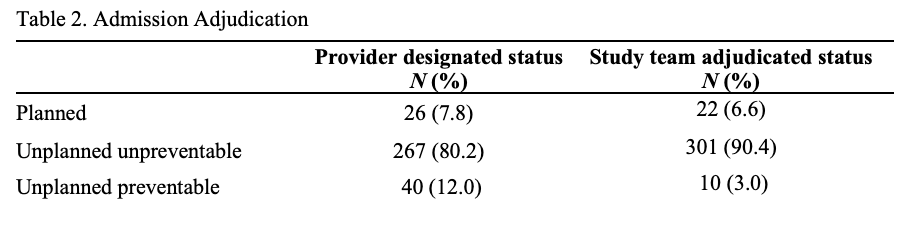
Description: We conducted an observational study using surveys that were automatically sent to the discharging provider at the time of readmission within 30 days of hospital discharge. We included all patients who presented for readmission from February 2, 2025 to June 25, 2025 after being discharged from the medicine service. We excluded admissions to medicine after discharge by non-general medicine teams including medical ICU, oncology, and surgery. During the study period, 401 surveys were automatically generated for readmissions within 30 days of discharge from general medicine teams at Duke University Hospital. The survey completion rate was 83.0%. Of the completed surveys, the readmissions were categorized by the discharging providers as 7.8% planned, 80.2% unpreventable, and 12.0% preventable. The study committee reviewed all surveys and found an 86.7% rate of agreement between the discharging providers and study committee adjudication. The study committee adjudicated the readmissions 6.6% planned, 90.4% unpreventable, and 3.0 % preventable (Table 2). The common themes among preventable readmissions included challenges with communications on discharge to skilled nursing facilities, missed opportunities to prescribe non-invasive ventilation on discharge for appropriate patients and readmissions without clear indication for hospitalization.
Conclusions: At a tertiary care academic medical center, we found that the vast majority of readmissions within 30 days were not preventable. Three quarters of the admissions that were initially thought to be preventable by the discharging provider were determined to be not preventable on further review by our study committee. Of preventable readmissions, key areas were identified for potential intervention. Other notable findings include high participation rate and strong engagement of inpatient medicine providers in working to understand the root causes of hospital readmissions. The limitations of this study include the subjective nature of adjudication and poor generalizability due to review of data from only one medical institution over a short time period. Further work is planned to expand this review to multiple hospital sites over an extended study period in order to further understand the common themes among patients with 30-day hospital readmissions.