Background: Since 2012, hospitals have been penalized for 30-day readmissions via the Hospital Readmissions Reduction Program. For fiscal year 2023, over 2000 hospitals were penalized for excessive 30-day readmissions, losing up to 3% of Medicare payments. Previous work has demonstrated that over 25% of hospital readmissions to general medicine were considered to be preventable when reviewed by a team of physician adjudicators. Mortality review surveys have been implemented and studied increasingly over the last few decades to identify preventable hospital deaths. We believe a similar model could be applied to the prevention of hospital readmissions.
Purpose: Our project aimed to better understand 30-day hospital readmissions to the general medicine services across our hospital system by gathering survey responses from the discharging provider. We assessed the proportion of planned and unplanned readmissions in addition to preventable and unpreventable readmissions. We also assessed characteristics of the index admission including the use palliative care consult, readmission risk scores and involvement of our complex case management teams to evaluate correlation with readmission risk.
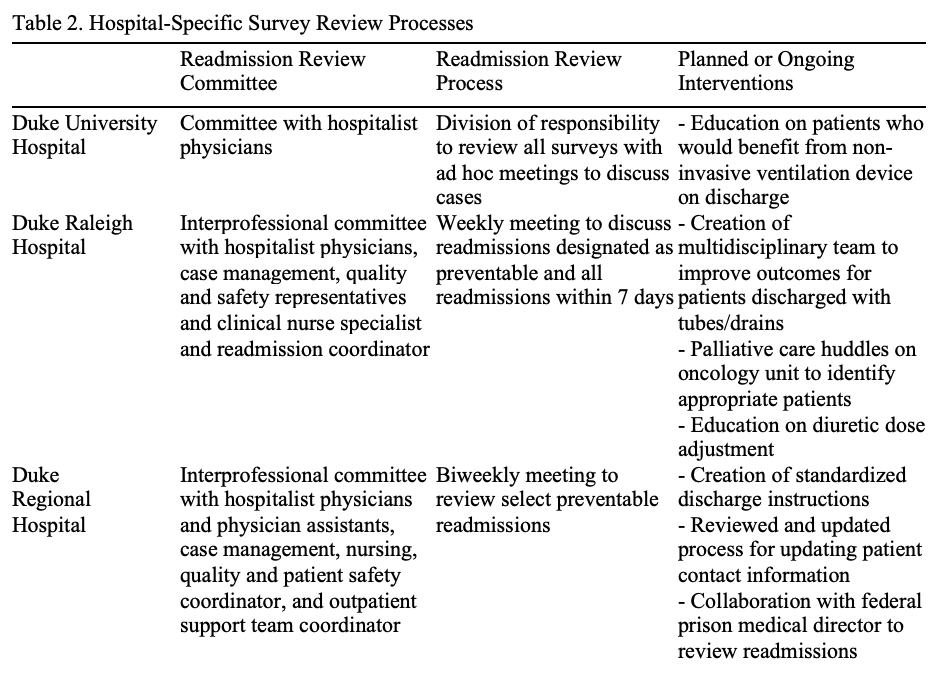
Description: From February 2, 2025 through July 31, 2025, 1267 patients were readmitted to the general medicine services across Duke University Health system after discharge from the same. Surveys were automatically generated and sent to the discharging provider from the index admission. Surveys asked providers to indicate if they believe the readmission was planned, unplanned and preventable or unplanned and unpreventable. The survey completion rate was 60.9%. Of the completed surveys, the readmissions were categorized by the discharging providers as 9.2% planned, 76.6% unplanned and unpreventable, and 14.2% unplanned and preventable. Of the readmissions felt to be preventable, the most commonly cited reasons were poor patient adherence to discharge instructions, medication-related issues, and social factors (Table 1). Each hospital site created readmission review committees to further evaluate preventable admissions but approached survey review with variable technique and created unique definitions of preventable admissions (Table 2). Several interventions have been created targeting root causes of preventable readmissions (Table 2).
Conclusions: The readmissions survey helped our hospital system to identify themes among 30-day hospital readmissions across three hospital sites. Although the majority of readmissions were not deemed preventable, all three hospital sites found areas for intervention to lower the rate of readmissions, which will benefit both our patients and our health system. There was variability in the survey review process and the composition of the multidisciplinary teams across our hospital sites. Multiple interventions have been implemented based on survey data to date. The survey completion rate was relatively high which demonstrates high engagement from our providers. Next steps for this process will evaluate impact on 30-day readmission rates and rates of preventable readmissions over a longer time period.
.png)