Background: Medication reconciliation (MR) is essential for safe and high-quality patient care, particularly with setting changes at admission and discharge.1 Prior studies have reported MR errors in up to 67% of patients at admission, with nearly 60% of these deemed clinically significant.2
Purpose: We aimed to innovate both the measurement and completion of resident-led MR at a major academic hospital. To do so, we conceived of new tools for both measurement and intervention. Before this project, no local instrument existed to measure time to completion of medication reconciliation, nor did any resource to provide standardized education on MR completion.
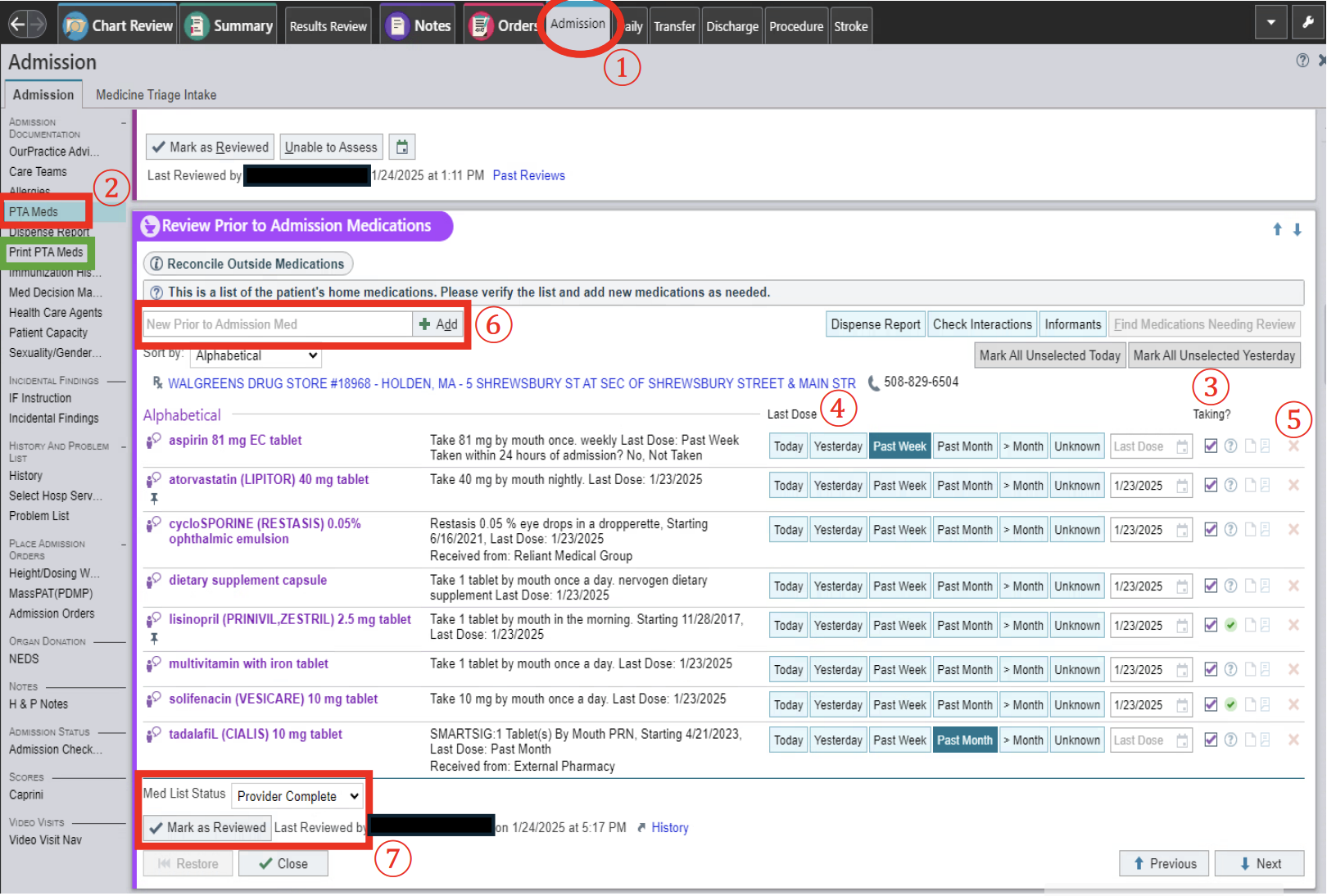
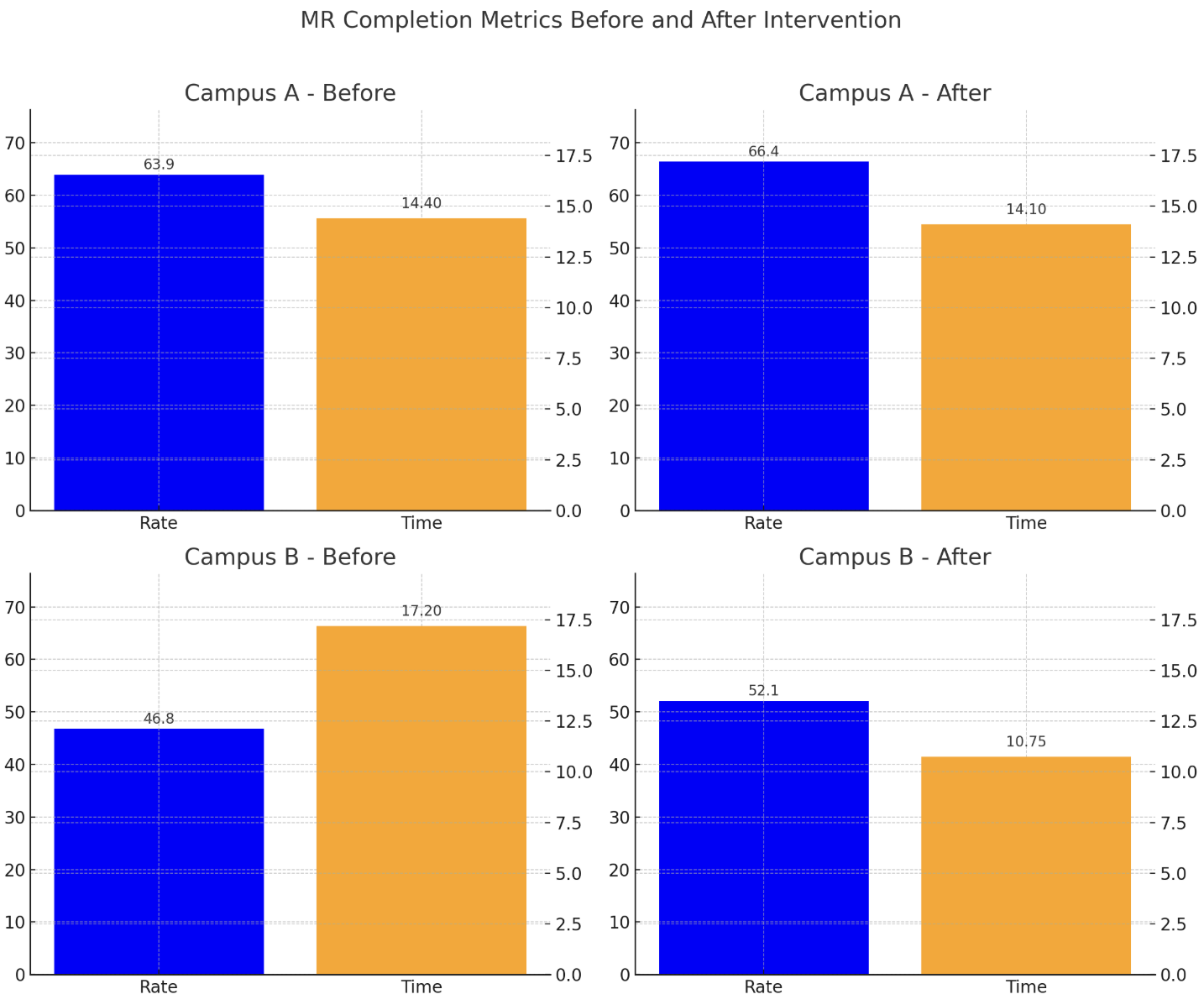
Description: We created a unique EMR-integrated report to assess MR completion for patients on resident acute care services. Both percent of patients with completion during admission and time-to-completion were measured. Data was collected longitudinally on resident-led admissions at our two campuses (herein A and B), stratified by admitting resident service specialty, during the three months before and after intervention. A baseline survey was conducted to assess knowledge of MR and perceived needs, informing the development and dissemination of our structured guide. The guide provided users with step-by-step instructions for completing MR in the EMR, troubleshooting common issues, and using pharmacy resources. A post-intervention resident satisfaction survey was conducted to guide further refinement.On initial survey 100% of respondents recognized MR as a critical component of the admission process, yet only 77.4% believed they consistently completed it while on wards. A majority reported that a standardized guide would improve completion rates and that additional pharmacy support would be beneficial. Post-intervention, 100% of respondents reported increased confidence and supported continued use of the MR guide, recommending deployment during residency orientation to enhance early adoption. Before intervention, MR completion rates were 63.9% at campus A and 46.8% at campus B, with average completion times of 14.4 hours and 17.2 hours after admission, respectively. Following intervention, completion rates rose to 66.4% and 52.1%, with modest reductions in average completion times to 14.1 and 10.75 hours. Between specialty-specific resident ward services, the pulmonology service achieved the highest MR completion rates while the hospital medicine-oncology service had the lowest.
Conclusions: MR at hospital admission is critical for error mitigation and quality of care. Despite this, completion rates remain a challenge at our hospital system and others. Medical trainees are often responsible for MR, and interventions to improve timely completion are likely to be of benefit. We suspect that this will likely contribute to safer, more reliable patient care.We find that early, structured MR education for trainees can modestly improve both completion rates and efficiency. Serial measurement of MR completion and time-to-completion with EMR-integrated tools supports tracking of performance and response to intervention. While our educational QI intervention improved MR performance, persistent barriers remain. Impaired patient communication, inadequate communication during inter-facility transfers, EMR heterogeneity, and time constraints remain common challenges. 3 A multi-disciplinary approach, particularly with pharmacy-supported MR, has been shown to reduce errors, enhance safety, and reduce operational costs. 4