Background: Re-expansion pulmonary edema (RPE) is a potentially life-threatening and feared complication of thoracentesis. While clinicians traditionally focused on avoiding rapid lung expansion by limiting drainage to less than 1.5 liters of pleural fluid, more recent literature suggests that monitoring pleural pressures using pleural manometry (PM) may allow for safe drainage of larger volumes. However, it is unclear if there are benefits to routine use of PM. We sought to assess the impact of routinely using PM during thoracentesis on the amount of fluid removed, including its effect on secondary outcomes including safety, post-procedure length of stay (PP-LOS), and 30-day readmission rate for repeat thoracentesis.
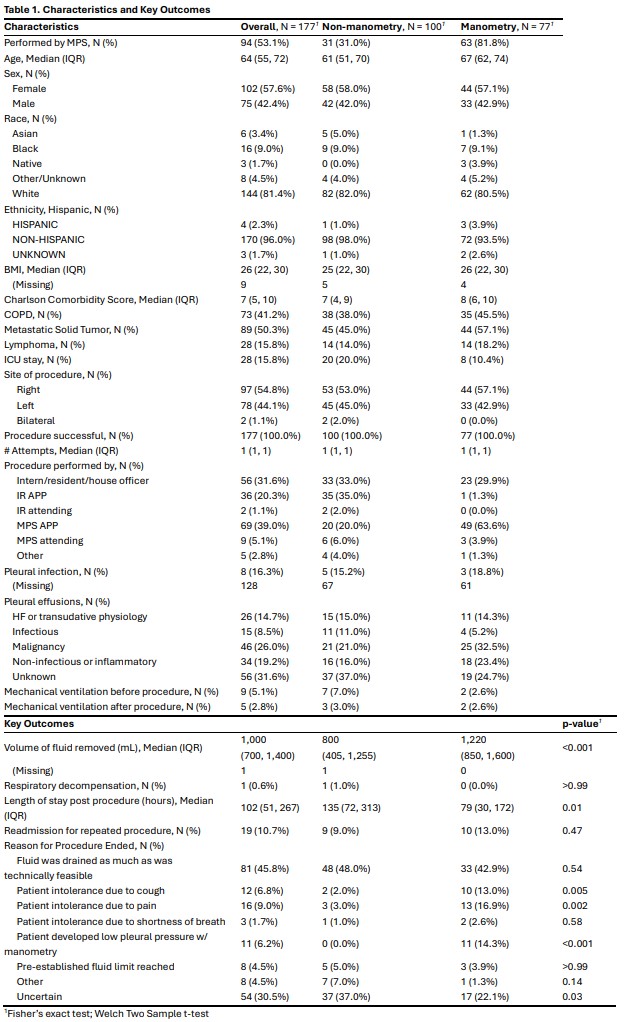
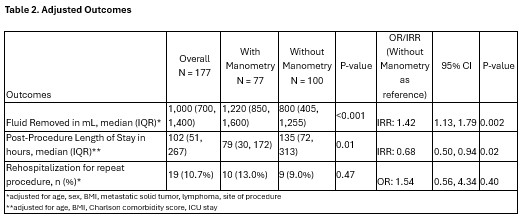
Methods: We retrospectively collected demographic and clinical data on adult patients who underwent thoracentesis at our 1,000-bed academic medical center between July 2021 and July 2023, including information on whether PM was used, amount of pleural fluid removed, and reason for terminating the procedure. The primary outcome was volume of fluid removed. Secondary outcomes were serious procedure-related complications (clinical RPE, iatrogenic pneumothorax requiring chest tube), PP-LOS and 30-day readmission rate for repeat thoracentesis. We assessed the association between PM and outcomes using negative binomial regression models, adjusting for age, body mass index, Charlson comorbidity score, intensive care unit stay, and procedure performance by the hospitalist medical procedure service.
Results: Of 177 patients who underwent thoracentesis, 77 (43.5%) patients underwent PM to guide fluid removal. Patients in the PM group were older (median [IQR], 67 [62-74] vs 61 [51-70] years old, p=.003) and had higher Charlson comorbidity scores (median [IQR], 8 [6-10] vs 7 [4-9], p=.003) compared to those in the non-PM group (Table 1). The median volume of fluid removed was higher in the PM group (median [IQR], 1220 [850-1600] vs 800 [405-1255] mL, p <.001). The rates of serious post-procedure complications were low in both groups, with similar rates of iatrogenic pneumothorax requiring chest tube (1 event in each group) and RPE (1 event in the non-PM group). PP-LOS was shorter in the PM group compared to the non-PM group (median [IQR], 79 [30-172] vs 135 [72-313] hours, p=.01). The 30-day readmission rate for repeat thoracentesis was similar in both groups (13% vs 9%, p=.47). In adjusted analyses, use of PM was associated with removal of larger volume of pleural fluid (IRR, 1.42; 95% CI, 1.13-1.79) and with shorter PP-LOS (IRR, 0.68; 95%CI, 0.50-0.94).
Conclusions: In this single center study, the use of pleural manometry was associated with larger volume of pleural fluid removed during thoracentesis and shorter post-procedure length of stay, with similar rates of serious procedure-related complications and 30-day readmission for repeat thoracentesis.