Case Presentation: A 33yo woman with sickle cell disease (SCD) from hemoglobin S Indianapolis requiring chronic transfusions presented with acute right sided chest, arm, and leg pain. There was initial concern for vaso-occlusive crisis, however her labs were less suggestive of acute crisis with Hgb near baseline (10 g/dL), total bilirubin of 1.7 mg/dL, absolute reticulocyte count near baseline (300 10^9/L ), and normal LDH. She had also received an exchange transfusion one week prior. Despite attempts at pain management, she continued to have severe pain in her RUE with associated numbness, tingling, and mild weakness. On re-examination she was noted to have a positive Hoffman reflex in her right hand, prompting concern for central neurologic causes of her pain. MRI of the cervical spine revealed C4-5 central disk protrusion and moderate right neuroforaminal stenosis as well as C6-7 right disk protrusion and moderate spinal canal stenosis (Figure 1). As the description of her symptoms followed the C4-C7 dermatome, it was concluded that her pain and numbness were likely from cervical disk disease and radiculopathy. The patient was started on pregabalin with improvement in her pain and she was weaned from IV opiates and discharged with close neurosurgery follow up.
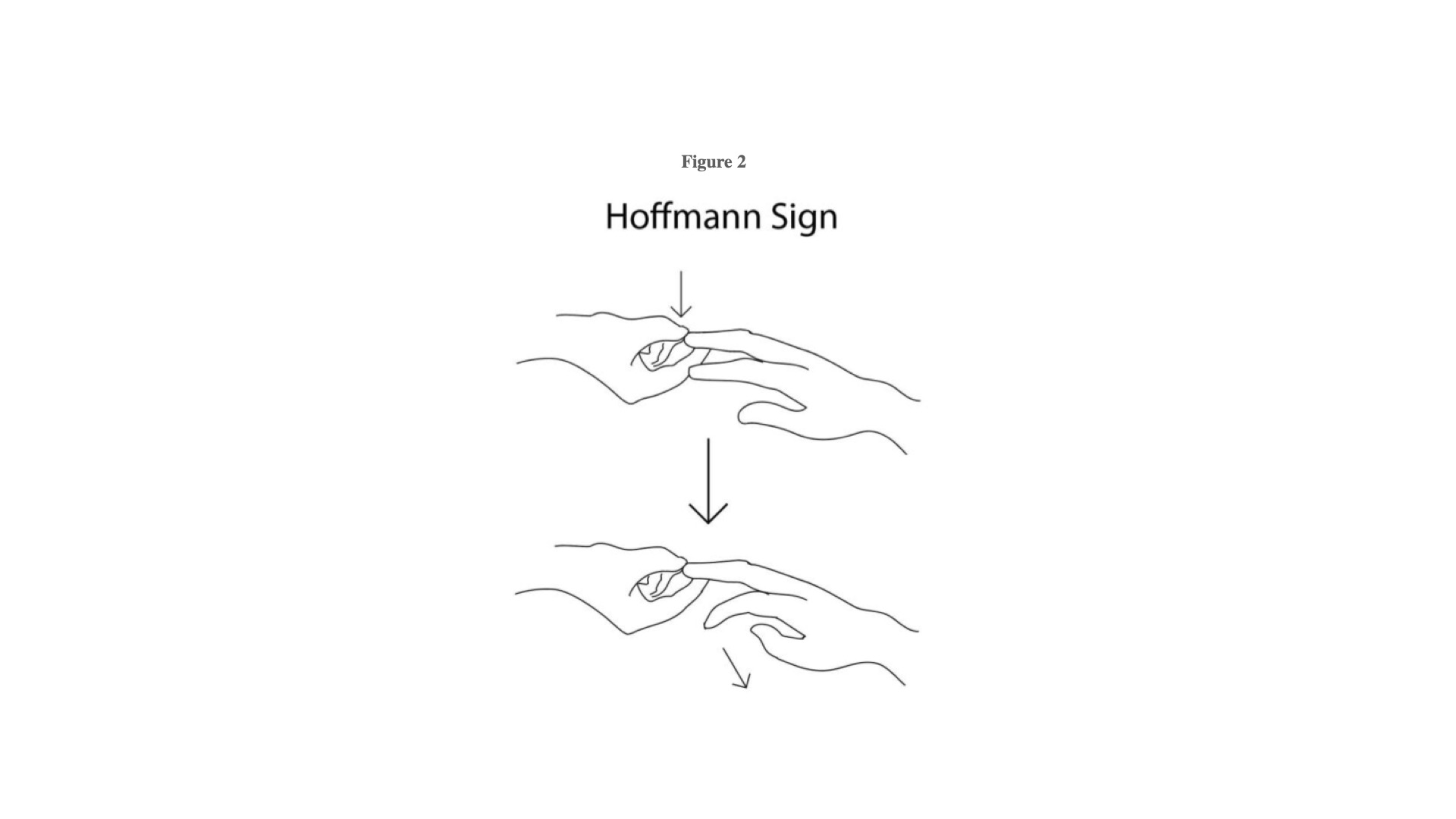
Discussion: Hospital practitioners should maintain a high index of suspicion for non-sickle cell related etiologies of acute neuropathic pain in patients with SCD. Sickle cell patients describe pain using both nociceptive (throbbing, crushing, cramping) and neuropathic (aching, cold, hot, shooting, stabbing) descriptors. Thirty percent of adult patients with SCD describe chronic neuropathic pain (1), which may cause anchoring bias in associating neuropathic symptoms to vaso-occlusion. In this case, a positive Hoffmans reflex increased the suspicion for an upper motor neuron (UMN) etiology of the patients symptoms and prompted further imaging confirming cervical disk disease. The Hoffmann’s reflex involves loosely holding the middle finger and flicking the fingernail downward, allowing the middle finger to flick upward reflexively. A positive response is seen when there is flexion and adduction of the thumb on the same hand (3).Our patient is relatively young to have cervical disk disease, which is more commonly seen in older patients; the mean age of diagnosis is 48 in women (2). SCD can cause a variety of pathologies in the spine secondary to marrow hyperplasia, tissue ischemia, and infarction from vaso-occlusion (4). Additionally, SCD Patients are more likely to develop vertebral osteomyelitis, compression fractures, degenerative changes, and osteoporosis (5). Our patient likely had acceleration of degenerative joint disease from underlying sickle cell disease resulting in cervical pathology more commonly seen in older patients. Clues that the patient was not experiencing a traditional vaso-occlusive event included: labs being at baseline without significant hemolysis, recent exchange transfusion, the description of unilateral and neuropathic symptoms, as well as the positive Hoffmans sign.
Conclusions: Hospitalists should maintain a high level of clinical suspicion for UMN disease in sickle cell patients presenting with neuropathic pain. Sickle cell disease causes early degenerative changes in the spine, and central nervous system etiologies of pain can be difficult to discern from typical vaso-occlusive crisis.
.jpg)