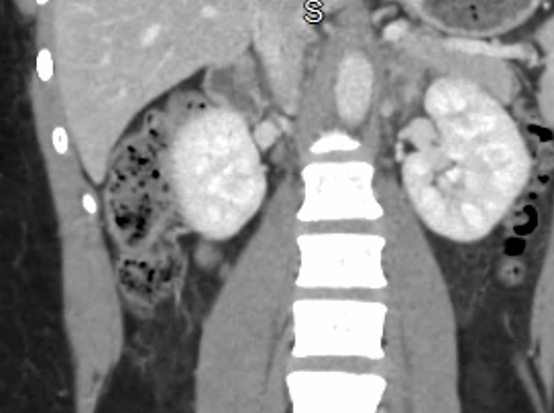
Case Presentation: n A 21-year-old woman with no significant medical history presented multiple times to the emergency department with severe headaches and markedly elevated blood pressures. Her initial episode involved a sudden 10/10 throbbing headache, nausea, and photophobia and was treated as migraine. A head CT subsequently revealed an intraparenchymal hemorrhage with thin subdural and subarachnoid components consistent with hypertensive emergency. During hospitalization, she developed malignant hypertension with chest heaviness and dyspnea. BNP was elevated, but troponin and chest X-ray remained normal. EKG demonstrated possible septal infarction with T-wave abnormalities, while transthoracic echocardiography showed no wall motion abnormalities. Despite metoprolol and hydrochlorothiazide, she continued to experience hypertensive crises, recurrent headaches, and new syncopal episodes. Given persistent severe hypertension in a young adult, evaluation for secondary causes was initiated. Renal duplex ultrasound was unremarkable. CT abdomen revealed a 4.7 × 2.8 cm right adrenal mass with washout characteristics of an adenoma. Plasma and 24-hour urine testing showed significantly elevated metanephrines and normetanephrines with normal VMA, confirming pheochromocytoma. Her blood pressure improved with amlodipine, spironolactone, carvedilol, and metoprolol. She established care with endocrinology and endocrine surgery and is pending adrenalectomy.
Discussion: Pheochromocytoma is a rare cause of secondary hypertension but may present dramatically with recurrent hypertensive emergencies. This case is notable for an initial presentation of intracranial hemorrhage—an uncommon but life-threatening manifestation of catecholamine excess. Hospitalists frequently encounter severe hypertension, and this vignette emphasizes the importance of maintaining suspicion for secondary causes, particularly in young adults with refractory hypertension or atypical symptoms.Elevated metanephrines remain the most sensitive biochemical marker, and this case highlights the diagnostic pitfall of normal VMA in confirmed pheochromocytoma. Early recognition and appropriate imaging can prevent repeated crises and end-organ injury.
Conclusions: This case demonstrates a severe presentation of pheochromocytoma resulting in hypertensive intracranial hemorrhage in a young adult. Early recognition of secondary hypertension by hospitalists is critical to prevent recurrent crises and end-organ injury. Lifelong follow-up remains essential due to risks of recurrence and associated hereditary syndromes
.png)