Case Presentation:
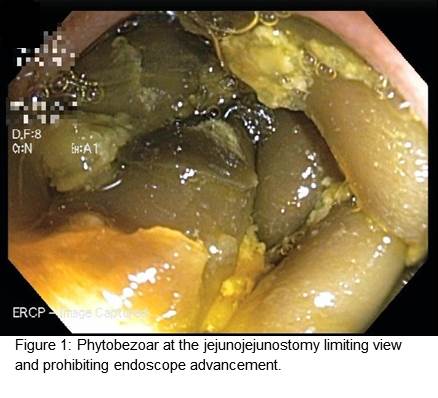
A 69 year old female with history of gallbladder cancer status post cholecystectomy/hepatic wedge resection with roux-en-y choledochojejunostomy and chemoradiation presents with recurrent abdominal pain and fevers of 102oF. She reports 2 prior episodes of bacteremia with no identified source. She was discharged 4 days ago after treatment for cholangitis with cefuroxime and metoclopramide, attributed to her surgically shortened biliary tree and radiation-induced biliary fibrosis. MCRP was unrevealing for pathology, and upper GI series showed no retrograde filling. On current presentation, she was febrile and tachycardic, with labs significant for alkaline phosphatase 639 U/L and total bilirubin 1.2 mg/dL. Cefepime was started and vancomycin added after 1/4 initial blood cultures grew gram-positive cocci; subsequent cultures were negative. ERCP discovered a large phytobezoar at the level of her jejunojejunostomy. Endoscopic disruption was incomplete but yielded a rush of biliary flow, and bowel prep was used to further fragmentation. Metoclopramide was discontinued given concern for obstruction at the level of hepaticojejunostomy (afferent loop syndrome), as pro-motility agents could drive food particulates to the bezoar and compound obstruction. Antibiotics were stopped upon relief of the obstruction with no subsequent signs of infection. It was revealed that the patient follows a vegetarian diet high in plant-based insoluble fiber. She was well at discharge off medications and on a low-fiber diet.
Discussion:
Bezoars were first harvested from goats and historically valued for purported medicinal properties; the term ‘bezoar’ is derived from Persian/Arabic words meaning antidote. Bezoars are hard masses that develop anywhere in the gastrointestinal tract (typically the stomach) from accumulated ingested material, including plant matter, hair, and extended-release medications. Gastric outlet obstruction, altered motility, prior surgery, and dehydration are risk factors for development. Diagnosis is typically made on endoscopy, though imaging may be helpful. Complications include bowel obstruction/perforation, obstructive jaundice, pancreatitis, and intussusception. Endoscopic fragmentation, chemical dissolution via Coca-Cola lavage, or cellulase enzymatic therapy are mainstay treatments. Patients should avoid high fiber diets, known precipitating medications, and bulk laxatives.
Conclusions:
This case highlights the role of diet in bezoar formation leading to the cholangitic picture of a patient with recurrent abdominal pain and fevers. A detailed history can increase suspicion for this extremely rare pathology. It is important to remember that multiple imaging modalities may not be sufficient to make a diagnosis without endoscopic evaluation.