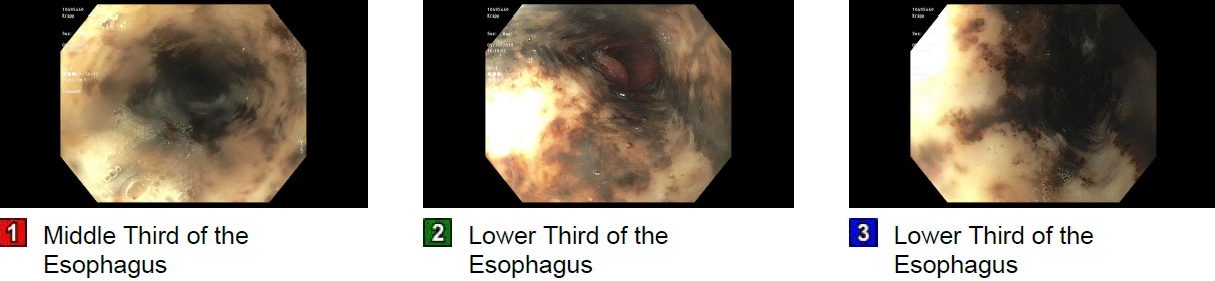
Case Presentation: A 61-year-old male with a history of alcohol abuse and Insulin-dependent diabetes mellitus presented with complaints of retrosternal chest pain and multiple bouts of coffee-ground emesis for three days. He reported a three-day binge of drinking vodka prior to the presentation. On examination, he was tachycardic, tachypneic, but normotensive. Hand and tongue tremors were observed. The abdomen was non-protuberant, non-tender with the absence of striae and caput-medusae. Initial laboratory workup revealed normal blood count, serum sodium (134 mEq/L), serum creatinine (1.53 mg/dl), blood urea nitrogen of 35 mg/dL, total creatine kinase (CK) of 2170 U/L, and transaminitis (AST 153 U/L, ALT 93 U/L). The patient was treated with normal saline, IV lorazepam, and phenobarbital due to concerns for alcohol withdrawal. In regards to hematemesis, the patient underwent an esophagogastroduodenoscopy (EGD), which unveiled diffusely congested and friable mucosa with black discoloration in the lower two-thirds of the esophagus consistent with the black esophagus (Figure 1). The black esophagus was conservatively managed with nil-per-oral (NPO), intravenous pantoprazole, and oral sucralfate. In the ensuing six days, the patient reported significant improvement in odynophagia and started tolerating oral feeds. He was discharged on oral pantoprazole with recommendations for repeat EGD in six weeks.
Discussion: “Black Esophagus” is a rare ailment with a reported incidence of 0.01 to 0.28%, with a male predominance (2). Though the exact etiology is unknown, an ischemic event is often described as the inciting factor, which increases the mucosal susceptibility to injury. Compounding factors include viral infections, sepsis, renal disease, diabetic ketoacidosis, and Stevens-Johnson syndrome. As per our knowledge, there is only one documented case of the black esophagus in association with excessive alcohol consumption (3). In the absence of a prior ischemic event, we postulate that isolated alcohol abuse precipitated our patient’s presentation. Upper gastrointestinal bleeding is the most common manifestation, often coupled with dysphagia, odynophagia, and chest pain. On EGD, a characteristic black necrotic discoloration of the esophageal mucosa is seen, frequently involving the distal two-thirds of the esophagus with sharp delineation at the level of the gastroesophageal junction (4). The mainstay of therapy includes intravenous proton-pump inhibitors (PPI) and treating the underlying cause. Stricture formation and esophageal perforations are notable complications in 25% and 7% patients, respectively. Due to underlying comorbid conditions, black esophagus confers overall mortality of 32% and disease-specific mortality of 6% (5). As such, a higher level of clinical suspicion amongst treating physicians can allow timely diagnosis and management of this rare entity.
Conclusions: Black esophagus is an uncommon presentation of esophageal necrosis which imparts significant morbidity and mortality. Alcohol use has been implicated in cases of hematemesis associated with erosive gastritis and Mallory Weiss tears, we suggest that physicians should mindful of rare etiologies such as black esophagus, which can be effectively managed with prompt therapy.