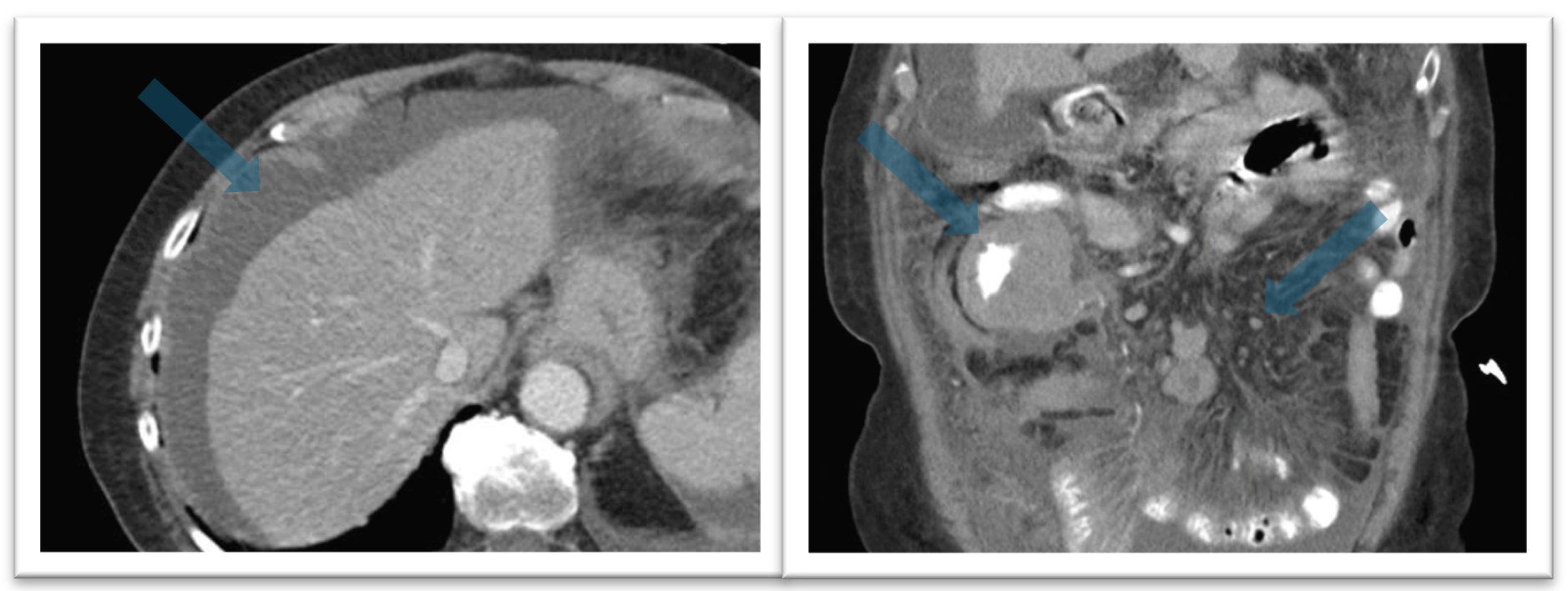
Case Presentation: An 84-year-old female with history of hypertension and hyperlipidemia presented to the emergency room with one month of vague, various symptoms, including right sided abdominal pain, decreased oral intake, loss of appetite, nausea, vomiting, generalized weakness, and fatigue. At baseline, she was healthy and enjoyed swimming and gardening. In August 2025, she started to develop neck pain, stiffness, and low-grade fevers. She saw her primary care physician and was prescribed doxycycline due to suspicion of a tickborne illness. Over the next 2 weeks, she developed generalized weakness, fatigue, right sided abdominal pain/swelling, nausea, vomiting, and unintentional weight loss of 20 pounds.On presentation, she was chronically ill appearing with decreased breath sounds at left base, severe abdominal distension, and RUQ/RLQ pain to palpation. She had leukocytosis and thrombocytosis. A CT abdomen/pelvis revealed gross thickening of the bowel in the RUQ, diffuse ascites, and pathologic lymph nodes in the mesentery (Figure 1). Abdominal paracentesis showed significantly elevated leukocyte count and monoclonal B-cell population consistent with B-cell lymphoma. She underwent excisional lymph node biopsy. The next day, her morning labs were significant for a uric acid of 16.5 and phosphorus of 6.6, consistent with tumor lysis syndrome. She was transferred to a tertiary care center for higher level of care. Her lymph node biopsy results and cytogenetic testing ultimately revealed a diagnosis of Burkitt Lymphoma.
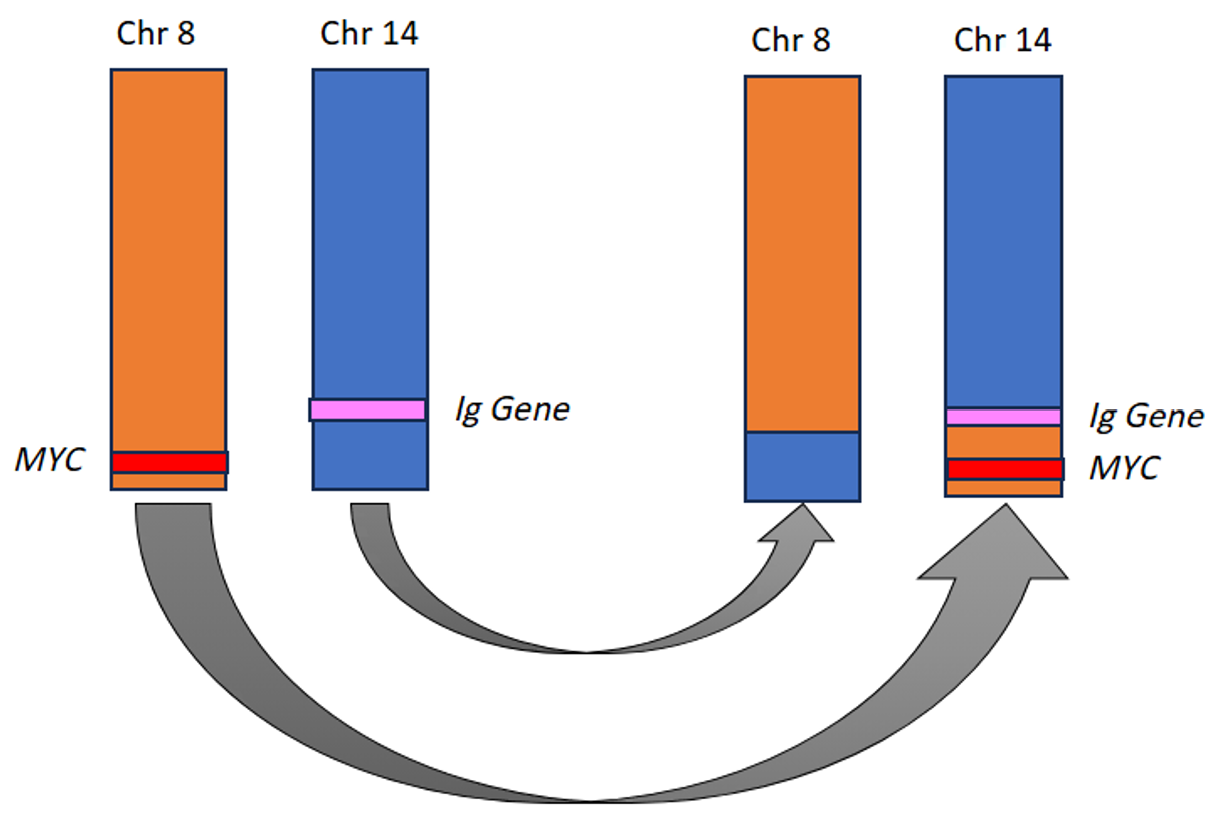
Discussion: Burkitt Lymphoma (BL) is a rare, aggressive, B-cell non-Hodgkin’s lymphoma. There are three variants of BL: endemic, sporadic, and immunodeficiency associated. BL is most commonly seen in children; however the sporadic and immunodeficiency variants can occur in adults. The endemic variant classically presents with a rapidly expanding jaw lesion, while the sporadic variant can present as a large abdominal mass (1). Patients with suspected BL should undergo lymph node biopsy with cytogenetics (flow cytometry, karyotyping, FISH) and PET/CT scan. Bone marrow biopsy and lumbar puncture are also indicated due to high rates of bone marrow and central nervous system involvement (1). The MYC translocation occurs in nearly all cases of BL, as overexpression of the MYC oncogene allows for unchecked progression through the cell cycle (Figure 2) (2–4). These mechanisms make BL one of the most aggressive lymphomas, with an average doubling time of 24-48 hours (2). Since BL is so aggressive, it requires high-intensity chemotherapy. Unfortunately, there have been no randomized controlled trials evaluating Burkitt lymphoma treatment in adults. The chemotherapy regimens for Burkitt lymphoma in adults have largely been adapted from regimens used for children (5). Due to the toxicities of these chemotherapy regimens, many older patients are unable to tolerate treatment. Prognosis of Burkitt lymphoma is highly dependent on age and functional status. 5-year overall survival in children/adolescents is 85-90% but decreases to 29-33% in adults >70 years-old (6,7).
Conclusions: Although commonly thought of as a childhood cancer, BL can occur in adults. It is one of the most aggressive lymphomas, in part due to the MYC translocation, and can present with B-symptoms and tumor lysis syndrome. Treatment requires high-intensity chemotherapy, and prognosis if poor in adults.