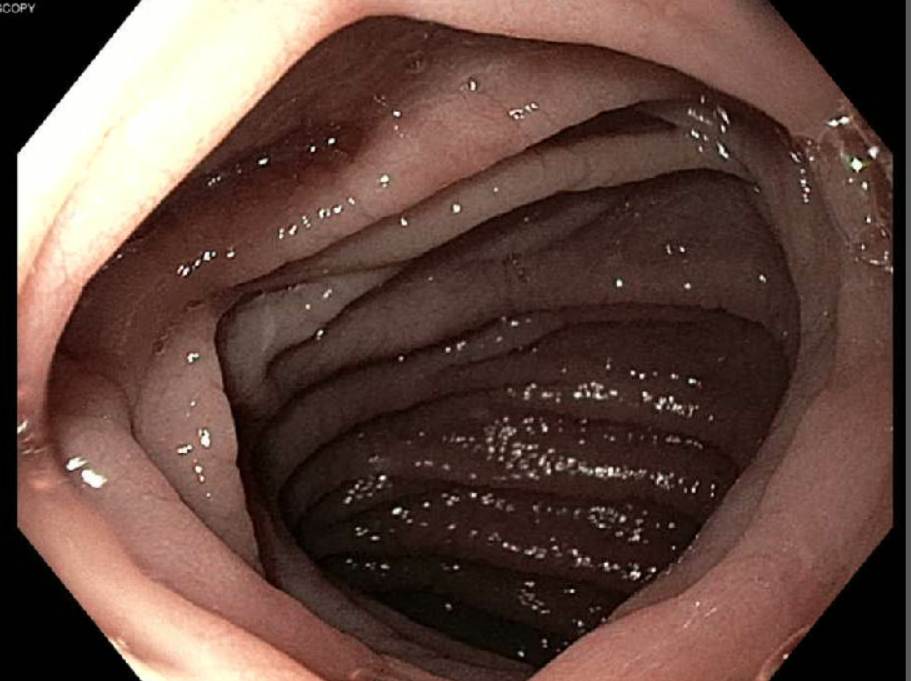
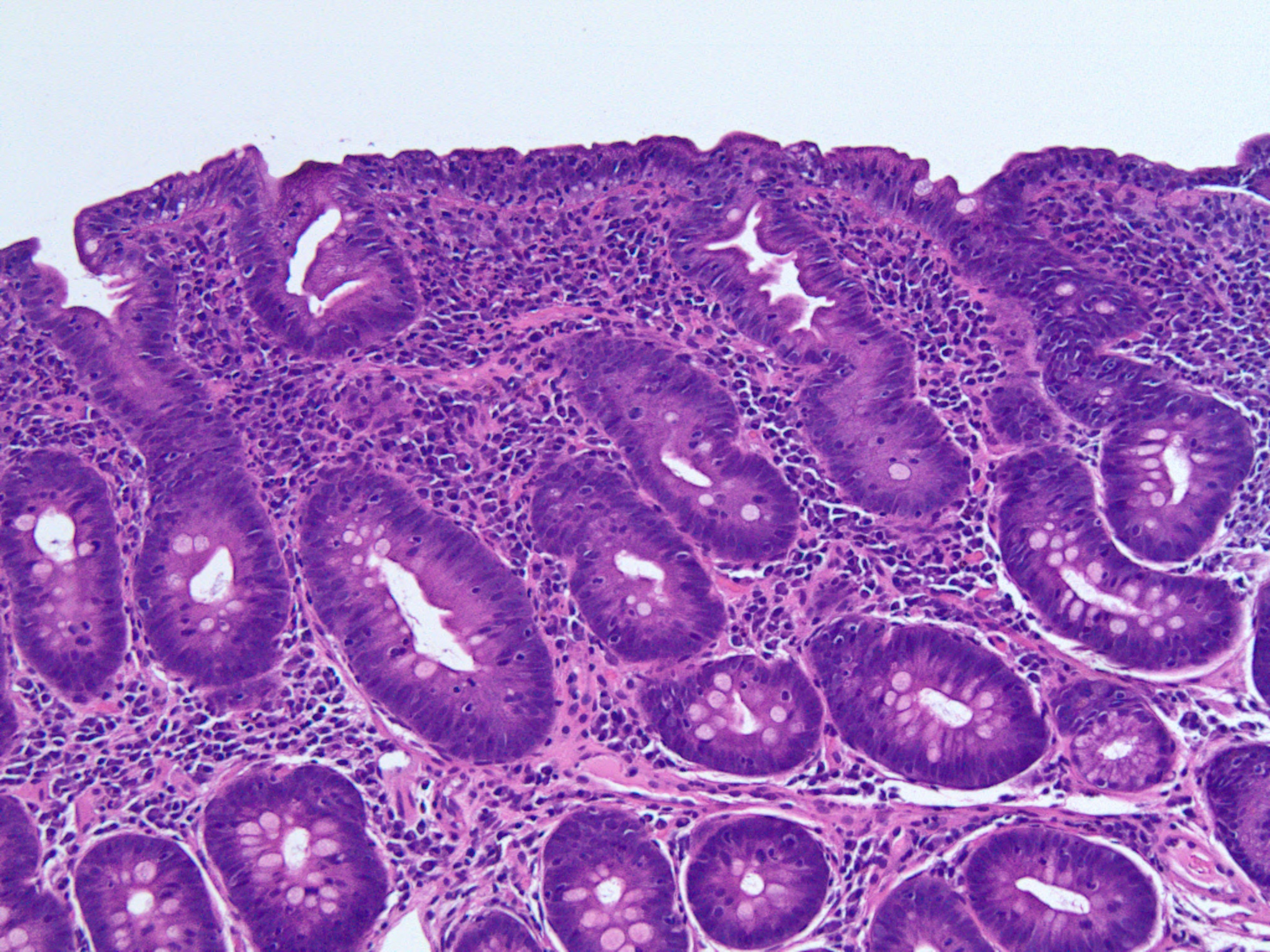
Case Presentation: A 20 year old male with past medical history of Type 1 Diabetes and Hypothyroidism presented to our hospital with severe hypocalcemia. His calcium was 5.8 mg/dl (normal range 8.6-10.3 mg/dl). His ionized calcium was 0.76 mmol/L (normal range 1.15-1.33 mmol/L). He had been complaining of generalized weakness for couple of weeks. Both of his parents had hypothyroidism. Vital signs were within normal limits. Physical exam was significant for positive Chvostek sign. Other labs revealed low magnesium, low potassium, low vitamin D, appropriately elevated Parathyroid Hormone, low albumin, metabolic acidosis and low ferritin. ). Renal function was normal. Computerized Tomography (CT)scan of abdomen revealed diffuse enteritis He was started on supplements for calcium, magnesium, potassium, vitamin D and iron. His electrolyte levels started improving after second day of hospitalizaton. Tissue transglutaminase antibody IgG was elevated. Upper gastrointestinal endoscopy showed scalloped and blunted duodenal mucosa. Duodenal biopsy showed villous blunting with intraepithelial lymphocytosis suggestive of celiac disease. He was started on gluten free diet. His symptoms improved and he was discharged home.
Discussion: Celiac disease is an immune mediated disease of small intestine characterized by malabsorption symptoms and villous atrophy precipitated by gluten protein. In most adult cases celiac disease presents as indolent course with gastrointestinal symptoms and nutritional abnormalities. Sometimes celiac disease can present as acute fulminant form called as celiac crisis. Celiac crisis is usually manifested by severe gastrointestinal manifestations, hypoproteinemia and metabolic and electrolyte disturbances requiring hospitalization. It is dignosed by criteria proposed by Jamma et al. In our case rapid onset of enteritis requiring hospitalization along with metabolic acidosis, hypoproteinemia and electrolyte abnormalities was sufficient for diagnosis of celiac crisis. Celiac crisis is a rare presentation of celiac disease and is associated with high morbidity and mortality. Few cases of celiac crisis have been reported. Most of the cases respond to gluten withdrawl and nutritional suport and few require steroids.
Conclusions: Sometimes celiac crisis can be initial manifestation of celiac disease like in our case hence clinicians should have high index of suspicion in someone presenting with gastrointestinal disturbances, hypotension, electrolyte and metabolic derangements after common causes have been ruled out.