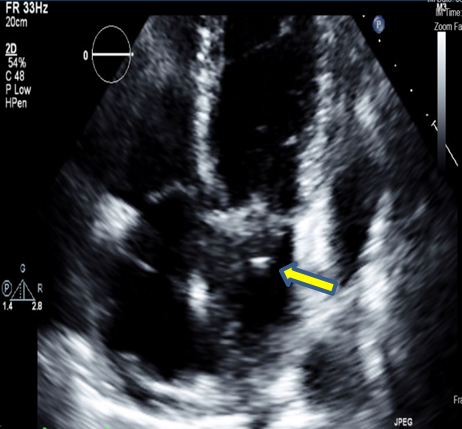
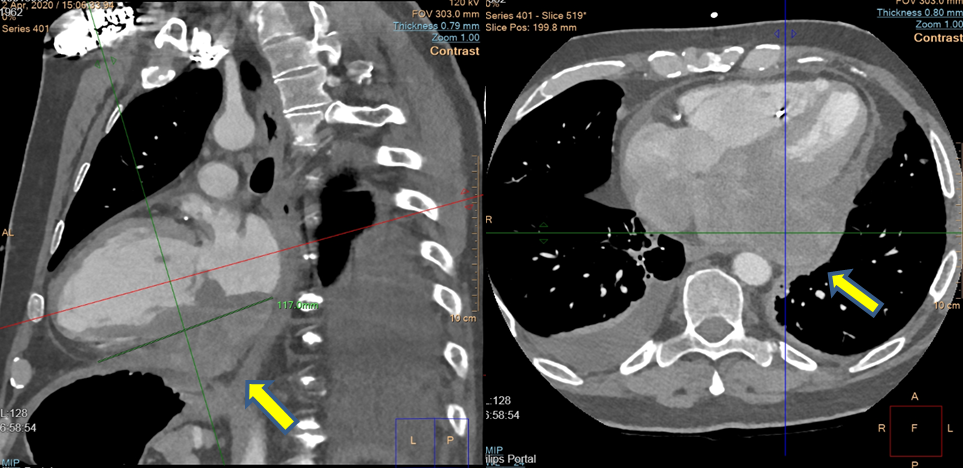
Case Presentation: A 58-year-old male with medical history of resected melanoma presented to our hospital with fatigue and exertional dyspnea of 1-week duration. He was found to have complete heart block and a large pericardial effusion. A dual chamber pacemaker was implanted, and pericardial drain was placed. The pericardial fluid was negative for malignancy and infection. After pericardial drain removal, the patient had repeat transthoracic echocardiogram that was concerning for a cardiac mass (figure 1).A cardiac computerized tomography (CT) showed large infiltrative mass of approximately 9 X 4 cm in size extending from the inferior left atrium to the apical inferior epicardial space. The tumor was infiltrating into the left ventricular inferior wall, interventricular septum and interatrial septum (figure 2).Given the history of resected melanoma, a whole-body positron emission tomography scan was performed and was remarkable solely for a hypermetabolic infiltrative mass in the inferior wall of the left ventricle. Brain magnetic resonance imaging (MRI) demonstrated no evidence of brain metastasis.Endomyocardial biopsy showed spindle cell sarcoma with negative lymphoma and melanoma markers. Given tumor size and location, patient was not a surgical candidate. He was referred to oncology service to begin chemotherapy.
Discussion: Cardiac sarcomas are the most common malignant primary cardiac tumors. Presenting symptoms vary based on tumor size and location. Fatigue, dyspnea and orthopnea are the most common symptoms. Other symptoms include dizziness, arrhythmias, heart blocks and pericardial effusion/tamponade. Due to nonspecific symptoms, early diagnosis of cardiac sarcomas might be challenging.Echocardiography remains the cornerstone of assessing cardiac tumors. However, having a large pericardial effusion that obscure an underlying mass might result in further delay in diagnosis.The presence of invasion and metastasis is usually assessed by cardiac CT and MRI. These techniques help with localization of the tumor and provide information regarding involvement of nearby structures and valves. Only a tissue sample can provide clear differentiation between benign and malignant cardiac tumors.Therapeutic options differ from patient to another based on tumor size, location, invasion and metastasis. Surgical resection is the gold standard therapy for patients without metastasis. Despite aggressive treatment, primary cardiac sarcomas have poor overall prognosis with median survival of 1 year.
Conclusions: This case emphasizes the importance of including cardiac tumors in the differential diagnosis of unexplained complete heart block and pericardial effusion. It also highlights the importance of repeating echocardiogram after pericardial fluid removal as the effusion may obscure visualization of underlying structures and masses.While CT and MRI can aid in localization of tumor and potential involvement of nearby structures, only tissue biopsy can confirm the diagnosis.