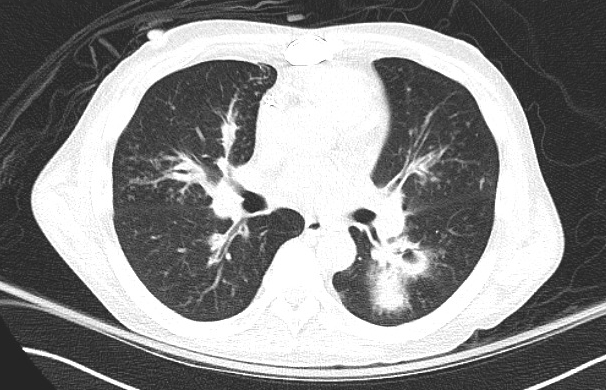
Case Presentation: A 50 year-old African American male with type 2 diabetes requiring insulin, end stage renal disease on peritoneal dialysis, coronary artery disease, infertility, chronic pancreatitis, alcohol use disorder, and recent influenza presented with fever and cough. He was afebrile, hypotensive, tachycardic, and tachypneic with a leukocytosis and bibasilar consolidations on chest x-ray. He was treated empirically for post-influenza bacterial pneumonia with vancomycin, cefepime, and azithromycin but remained tachycardic and tachypneic. CT chest showed bronchiectasis and multifocal cavitations with ground glass opacities surrounding consolidation (“halo sign”). The halo sign is associated with numerous infections, such as mucormycosis, cryptogenic organizing pneumonia, and Mycobacterium tuberculosis, but given that beta-D-glucan was greater than 500 pg/mL, aspergillosis was suspected. He underwent bronchoscopy with bronchoalveolar lavage (BAL) and endobronchial biopsy. After the procedure he was intubated for hypoxemic respiratory failure. Meropenem and voriconazole were started.Blood cultures grew burkholderia cepacia, and respiratory cultures grew B. cepacia, candida albicans, and aspergillus fumigatus. Biopsy revealed focally invasive aspergillus. Despite escalation to meropenem, amphotericin, and vancomycin, he had persistent fever, tachycardia, hypotension, and airway obstruction from hemoptysis. He expired due to recurrent cardiac arrest.Autopsy showed lung and pancreatic features strongly suspicious for a cystic fibrosis transmembrane conductance regulator mutation. Cause of death was identified as invasive pulmonary aspergillosis (IPA) complicated by pulmonary hemorrhage and B. cepacia pneumonia.
Discussion: Clinical manifestations of IPA include cough, fever, pleuritic pain, and hemoptysis. Imaging classically reveals a halo sign, which can indicate pulmonary infarction surrounded by alveolar hemorrhage. IPA is the most common pulmonary infection associated with a halo sign in immunocompromised patients. Diagnosis is confirmed with biopsy. IPA primarily occurs in severely immunocompromised patients; notably, the patient in this case did not have a known cause of severe immune compromise. One likely cause is undiagnosed cystic fibrosis (CF). CF should be suspected in adults with recurrent pulmonary infections, male infertility, pancreatitis, nasal polyposis, and malabsorption. In one large study, 7% of individuals with CF were diagnosed at age > 18. This patient was African-American, and CF is relatively rare in black individuals (1:15,000). Late onset phenotypes are even rarer. CF unifies this patient’s history (chronic pancreatitis and infertility) and lung pathogens (Burkholderia and Aspergillus). Although autopsy suggested CF, confirmatory genetic testing was not obtained.
Conclusions: Atypical causes of pneumonia should be considered in patients without improvement on broad spectrum antibiotics. Early testing, such as BAL and endobronchial biopsy, should be pursued. Clinicians must maintain a high level of suspicion for immunocompromised states that can lead to opportunistic infections and rare pathogens, such as CF. Late onset CF should also be considered in patients with cavitary lung lesions and bronchiectasis.