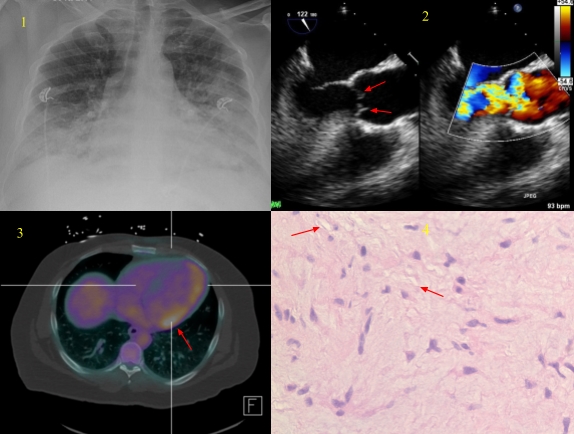
Case Presentation: A 39-years-old male with a history of hypertension presented with a one-month history of worsening shortness of breath associated with orthopnea, paroxysmal nocturnal dyspnea, and leg swelling. He denied fevers or chills, but he did report night sweats. On the day of hospitalization, he developed significant shortness of breath at rest associated with coughing white to pinkish mucus. He was in acute respiratory distress with oxygen saturation 72% on room air. Cardiopulmonary examination revealed regular heart rate, rhythm, no murmur, crepitations were heard in bilateral lung fields. Jugular venous distension was noted, pitting edema was present in bilateral lower extremities. The rest of the exam was unremarkable.His blood workup showed normal complete blood count, mildly elevated troponin (0.06 ng/ml), elevated BNP (250 pg/ml), CRP (3.4 mg/dl), and ESR (59 mm/hr). Electrocardiogram showed sinus tachycardia but no significant ST-T changes. CXR showed asymmetric interstitial infiltrate (Figure 1). A CT of the chest with contrast ruled out pulmonary embolism and aortic dissection. A transthoracic echocardiogram revealed severe aortic insufficiency (AI) with normal EF, a subsequent transesophageal echocardiogram (TEE) showed severe aortic insufficiency, and small masses on the ventricular side of the right and noncoronary cusps, interfering with the coaptation of the valve and causing severe AI (Figure 2). Subsequent cultures were negative for endocarditis and nuclear medicine myocardial perfusion study was strongly suggestive of cardiac sarcoidosis (Figure 3).
The diagnosis was initially uncertain as our patient did not have a history of trauma, infective endocarditis, sarcoidosis, rheumatic fever, syphilis, bicuspid aortic valve or Marfan’s syndrome. He underwent aortic valve replacement with a bioprosthetic valve. Histological examination of the aortic valve showed myxoid degeneration but no granulomas (Figure 4). He was doing well one year after surgery.
Discussion: Myxoid degeneration of aortic valve was first described in 1957, although less commonly affected than mitral valve, it is still a common cause of severe aortic valve regurgitation especially if certain underlying cardiac conditions such as a history of infective endocarditis, rheumatic heart disease, congenital heart disease, and Marfan’s syndrome are present. Myxoid degeneration can involve normal aortic valve. However, myxoid aortic regurgitation of uncertain origin usually affects male patients in their 7th decade of life, who have a history of long-standing hypertension and coronary artery disease. Our patient’s young age of presentation is atypical although he fulfills certain risk factors.
Conclusions: Myxoid degeneration is a rare cause of acute aortic valve regurgitation in young age. The diagnosis requires histopathological identification of acid mucopolysaccharide deposition and disruption of the valve fibrosa. Echocardiogram has limited value in the identification of myxomatous aortic valve. We should be aware of the myxoid degeneration that can present as acute aortic regurgitation in a younger age group. Aortic valve replacement is the definitive treatment as myxoid degeneration is a progressive disease.