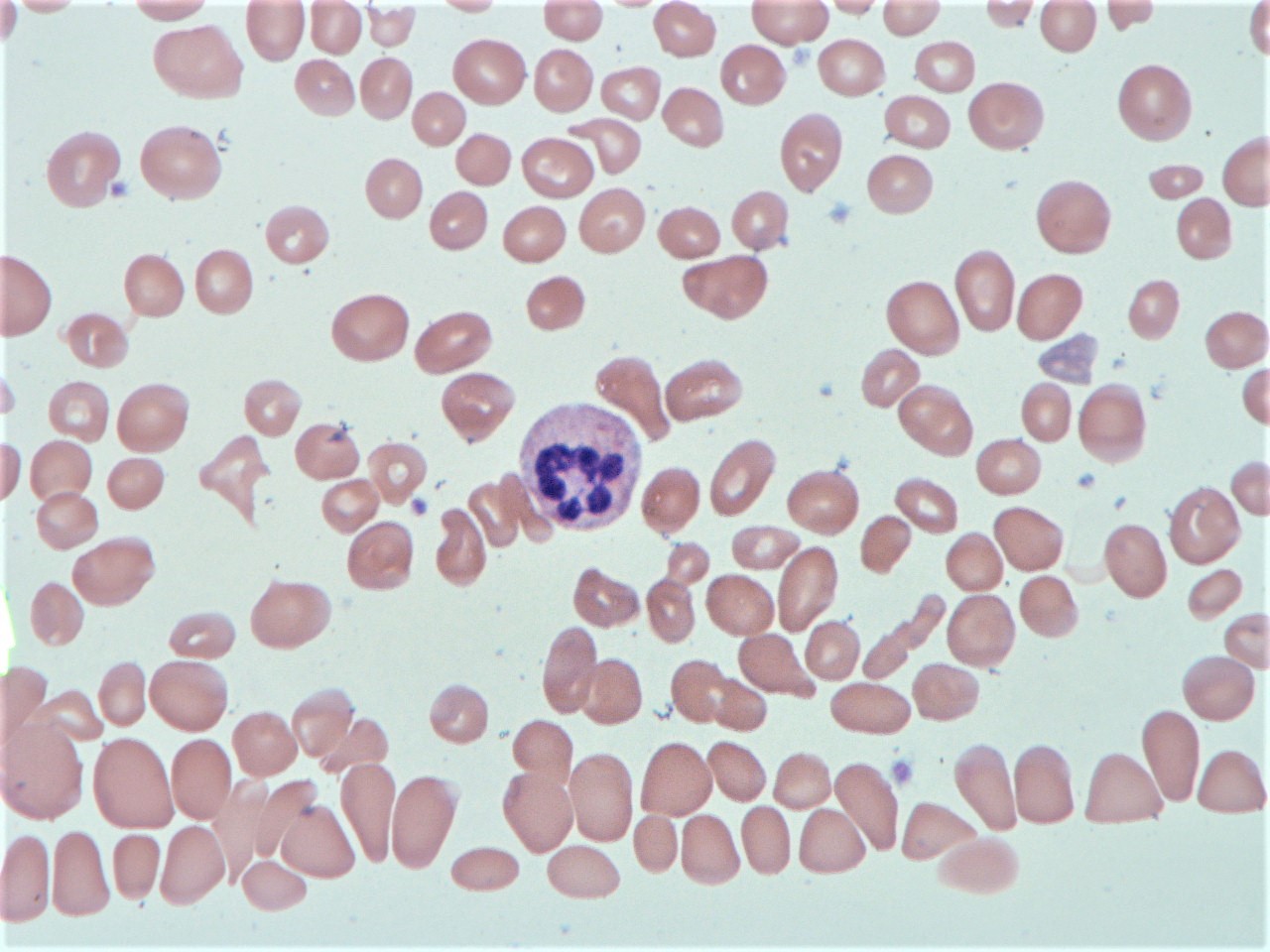
Case Presentation: A 75 year old woman with past medical history of hypothyroidism presented with weakness and the sensation of “large folds of skin” on the bottom of her feet. Pertinent physical exam findings included conjunctival pallor, nonspecific diffuse abdominal tenderness, and hyperpigmented macules of the dorsal finger tips and soles, which were also new since the onset of weakness.Initial lab results were significant for pancytopenia: platelets 68, white blood cell count 2.7, and hemoglobin 5.2 with an MCV of 119. The patient was admitted for work up of anemia and was treated with 2 units of packed red blood cells. Subsequent labs revealed vitamin B12 <60 and normal folate. She had evidence of hemolysis (decreased haptoglobin, LDH 2558) and an increased absolute reticulocyte count, but her Coombs test was negative. Peripheral smear revealed macrocytic normochromic anemia with anisopoikylocytosis, leukopenia with hypersegmented neutrophils, thrombocytopenia without blasts (Figure 1). Given new onset of rash on palms and soles, an RPR was ordered which was negative. With the presumption of B12 deficiency, and given the initial severity of the deficiency, the patient was treated with a regiment of intramuscular B12 injections. Final labs after discharge revealed positive antibodies to intrinsic factor and parietal cell, thus confirming the diagnosis of pernicious anemia in our patient.
Discussion: Vitamin B12 deficiency is a common cause of megaloblastic anemia and may be accompanied by various neuropsychiatric symptoms. It is most commonly due to autoimmune gastritis, or pernicious anemia. Diagnosis can be made with serum B12 <350 pg/ml (90% sensitive), anti-intrinsic factor antibody (50% sensitive, 100% specific), and anti-parietal cell antibody (80% sensitive, 50-100% specific) (1). Although most B12-deficient cases have only mild findings, 10% of patients may develop symptomatic pancytopenia, severe anemia and less commonly hemolytic anemia (about 1.5% of cases) (2). In cases of severe pancytopenia and hemolysis in elderly patients, there may be suspicion for malignancy or leukemia, but bone marrow biopsy and aspiration are not necessary and may confuse the diagnosis.B12 deficiency may present with peripheral neuropathy, areflexia, and loss of proprioception and vibratory sense. Hyperpigmentation is rarely reported as the presenting manifestation of B12 deficiency, but the rash is characterized as hyperpigmented macules of the extremities with a predilection for the dorsum of the palms and soles, as well as accentuation over the interphalangeal joints, as seen in our patient (3, 4). When patients present with severely low levels of B12, intramuscular administration can be considered for rapid improvement of symptoms, although oral administration of high-dose vitamin B12 (1 to 2 mg daily) is just as effective (5).
Conclusions: This vignette describes an uncommon case of B12 deficiency presenting with severe hemolysis and new onset hyperpigmented rash of the palms and soles. Clinicians should maintain a wide differential when evaluating pancytopenia in an elderly patient, but characteristic peripheral smear and negative hemolysis work up should be reassuring for B12 deficiency.