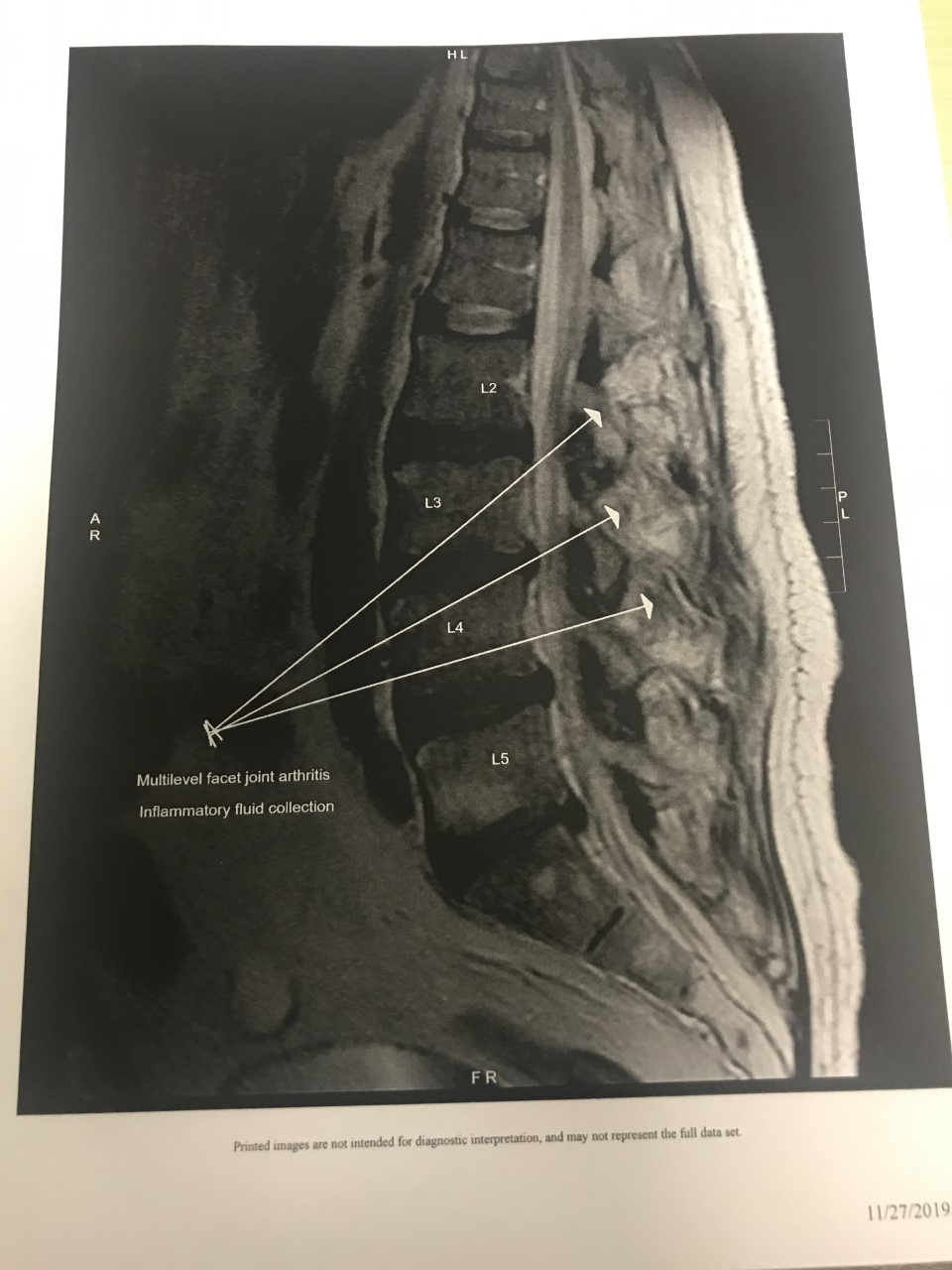
Case Presentation: 60-year-old African American male with history of polyarticular tophaceous gout, chronic back pain related to DDD, HTN, CKD stage III, HIV on HAART, COPD presented with worsening back pain of 1-week duration associated with progressive lower extremity weakness and inability to walk. Low back pain was noted as sharp, stabbing in nature radiating down his left leg.Physical exam revealed an afebrile, nontoxic obese man with lower back tender to palpation and bilateral lower extremity weakness, unable to stand or walk. Straight leg raising test on left was limited because of pain. lab data; wbc of 9.9, ESR of 75 & high CD4 count and HIV viral load <20.Vital signs; significant for fever of 100.2 on initial presentation. Strength testing significant for left hip flexion 3+/5, right hip flexion 4/5, Left thigh abduction 4-/5, right thigh abduction 4/5, left thigh adduction 4-/5, right thigh adduction 4/5 and left knee flexion & extension 4-/5, right knee flexion & extension 4/5. upper extremity strength 5/5 equal bilaterally. MRI of lumbar spine done at outside facility, showed inflammatory changes and fluid collections posterior to the bilateral L1-2 through L4-5 facets with multilevel septic facet arthritis, abscess and epidural enhancement at L2-5 with no fluid. This was read as concerning for discitis and paraspinal abscess. He was empirically started on broad spectrum antibiotics. On presentation, he had CT guided aspiration of fluid from right L4-L5 facet joint and aspirated fluid was sent for culture with no growth. Three days later, he developed bilateral knee pain with swelling and fever concerning for acute gout. Range of motion of knees was very limited. ESR and CRP were elevated to 95 and 34.67, respectively. Serum uric acid was elevated to 11.9. Given no clinical improvement and antibiotics and cultures negative, the joint fluid previously aspirated was tested for monosodium urate crystals and was positive. After the initiation of Prednisone, the patient’s back, knee, and leg pain improved along with his mobility improved. He had mildly limited functional mobility at discharge requiring ongoing home health for physical therapy. He was discharged with prolonged steroid taper. Acute gout was deemed as the cause of his back pain and Leg weakness.
Discussion: Back pain with leg weakness is a common problem needing hospitalization. Common causes include spinal arthritis, disc herniation, spinal cord root compression, infectious discitis, spinal abscess, spinal canal stenosis, etc. In this case, MRI of lumbar spine showed inflammatory changes including facet joint arthritis and paraspinal fluid collection. Cultures sent from joint fluid aspiration were unrevealing, but testing for monosodium urate crystals and recognition of knee inflammation as acute gout helped clinch the diagnosis.
Conclusions: Gout can mimic multiple diseases. In patients with prior history of tophaceous gout and chronic kidney disease presenting with back pain and leg weakness and/or radiculopathy, a high index of suspicion is needed for diagnosis of spinal gout. Early diagnosis and treatment may spare a patient from needing surgery.