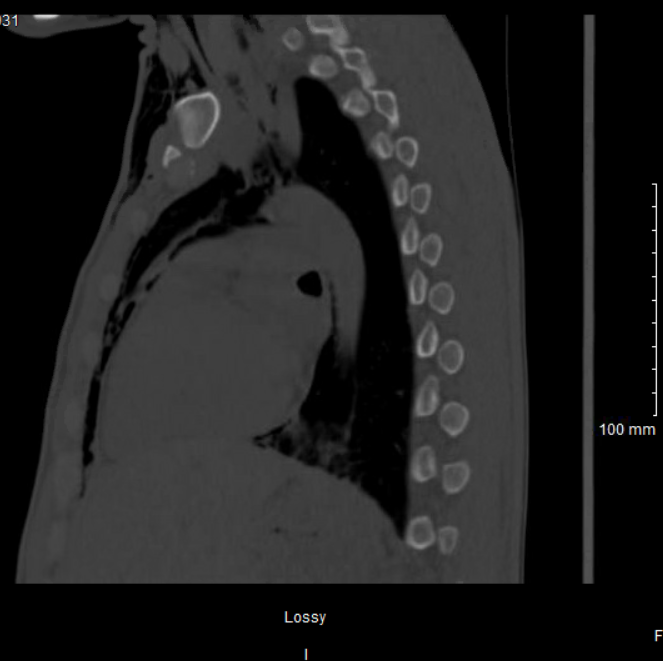
Case Presentation: A 32-year-old male with a past medical history of COVID-19 infection, type 1 diabetes mellitus, repeated episodes of diabetic ketoacidosis (last 6 days prior), S. aureus bacteremia, rhinotillexomania, and medical non-compliance presented with acute onset facial and neck swelling and pain. On admission, a CT of the facial bone demonstrated extensive soft tissue emphysema of the face and a fracture of the right lamina papyracea. The patient denies any history of trauma, chest pain, shortness of breath, or drug use. A chest x-ray shows extensive subcutaneous emphysema with pneumomediastinum and pneumopericardium, new compared to a chest x-ray completed 5 days prior. A CT esophagogram showed no evidence of barotrauma and the interval development of the right lamina papryacea fracture from a head CT one month prior, our team suggested the air within the soft tissues is attributed to the ethmoid fracture and exacerbated by repeated nose blowing. His condition was conservatively managed with sinus precautions, and continuation of his current course of antibiotics for his bacteremia. Repeat chest x-ray and CT chest after 3 days of admission showed improvement, and the patient was discharged on day 4.
Discussion: Subcutaneous emphysema (SE), pneumomediastinum (PM), and pneumopericardium (PC) can occur due to a myriad of different etiologies. Defined as air introduced into the fascial planes, SE can be traumatic, surgical, iatrogenic, or spontaneous in onset. Typically, a perforation within the gastrointestinal or respiratory tract complicated by emesis, coughing, or Valsalva maneuver results in air forced into the subcutaneous tissues, pericardium, mediastinum, or retroperitoneal space. More rarely, air descends from maxillofacial structures causing these pathologies. This patient’s complicated clinical picture reveals multiple potential etiologies for his triad of clinical findings. There are reports of PM and spontaneous SE as a rare complication of diabetic ketoacidosis. [1] Typically resulting from alveolar rupture secondary to changes in pressure gradients from vomiting and/or Kussmal respirations allowing air to move along the bronchovascular bundle. [2] This patient also has a history of medical non-compliance and is a known poor historian, so we cannot completely rule out trauma to the face or cocaine use, which have also been associated with PM. [3]
Conclusions: This case describes a rare triad of clinical findings which may arise in hospital medicine settings as a delayed result of facial trauma. Most likely, this patient’s repeated digital manipulation of the nose caused erosion, followed by fracture to the medial lamina papyracea, a fragile bone on the medial orbital wall. [4] Rathore, et. al reports a case of medial orbital wall erosion secondary to rhinotillexomania complicated by MSSA infections to the soft tissue in the medial orbit. [5] Fractures of the medial orbital wall and ethmoid sinus are more frequently associated with SE than other fractures of the midface. [6] The fracture acts as a ball-valve mechanism, trapping air within the fascial layers. This patient has been known to repeatedly blow his nose as part of his rhinotillexomania, which has been shown to force air into the subcutaneous tissues in the setting of maxillofacial injuries. [7]