
Case Presentation: 21-year-old female presented with three weeks of progressive right-sided chest pain, shortness of breath, and fatigue. Her symptoms began shortly after a three-hour car ride. She had a history of a second-trimester miscarriage four months earlier, complicated by acute blood loss anemia requiring transfusion. She briefly used oral contraceptives following the miscarriage. She denied smoking, alcohol, or drug use, and had no personal or family history of clotting disorders. On presentation, she was tachycardic at 130 bpm, mildly febrile, with an oxygen saturation of 92% on room air. Physical exam revealed tachycardia, mild tachypnea, and decreased breath sounds at the right lung base.Initial labs revealed a hemoglobin of 9.0 and a white blood cell count of 13,000 with a neutrophil predominance. High-sensitivity troponin was elevated at 53.ECG showed sinus tachycardia with non-specific ST-T wave changes. Chest X-ray revealed a right lower lobe infiltrate. CT angiogram of the chest demonstrated large pulmonary arterial filling defects involving branches to the right lower lobe, right middle lobe, and left lower lobe. There was also a moderate pericardial effusion. A duplex ultrasound of the lower extremities showed no evidence of deep vein thrombosis (DVT).
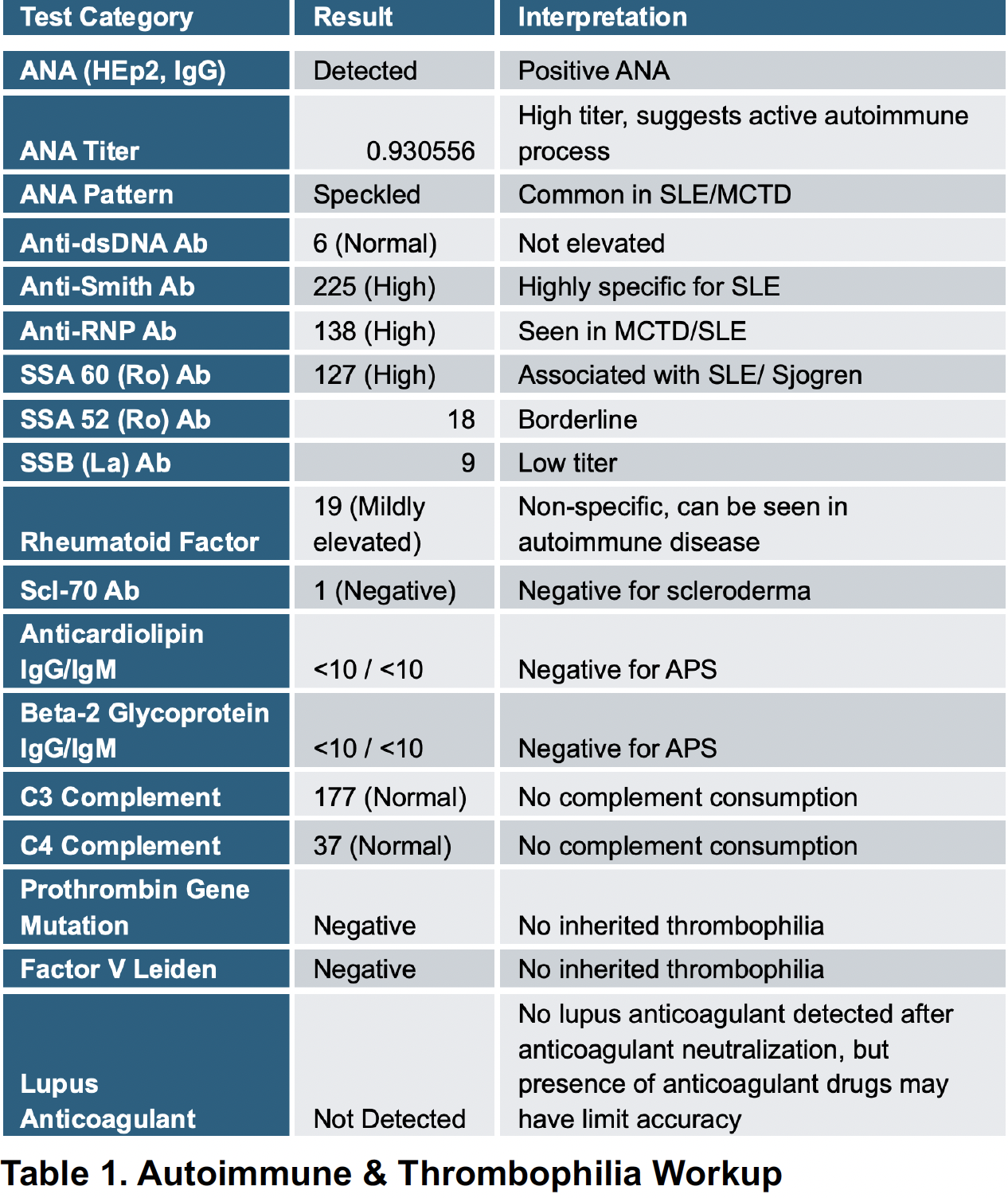
Discussion: This is a diagnostically challenging scenario of an otherwise healthy young woman with a large, spontaneous pulmonary embolism whose subsequent workup disclosed serological data highly suggestive of underlying Systemic Lupus Erythematosus. Failure to present with characteristic SLE features such as malar rash, photosensitivity, arthritis, or overt renal impairment is indicative of the “latent lupus” phenomenon or a prodromal, non-specific variant of the disease in which the thromboses can be a presenting and possibly isolated dominant feature [1,2].The diagnostic pathway of this case highlights the necessity for a high index of suspicion for autoimmune disorders in young patients, particularly in women, who experience an unprovoked VTE. While our patient presented with compelling immunologic evidence (high ANA, anti-Smith, anti-RNP, anti-SSA), she lacked sufficient concurrent clinical criteria at presentation to satisfy these classifications. However, the existence of anti-Smith antibodies is highly specific for SLE (>99% specificity) [3], and this nearly ensures that she was at least in an early stage of the disease or had a latent variety of lupus that predisposed her to thrombosis.
Conclusions: This case describes an unprovoked pulmonary embolism in a young woman as the initial presentation of what is highly likely an underlying, previously inactive systemic lupus erythematosus (SLE). The detection of highly specific autoantibodies (anti-Smith) in the absence of classic clinical features highlights the importance of a comprehensive autoimmune evaluation in young patients presenting with unexplained thrombosis, even without traditional risk factors or overt autoimmune symptoms. Recent hormonal exposures and pregnancy-related complications may have acted as triggering factors in the setting of an underlying autoimmune predisposition. Early recognition and close follow-up are essential to confirm the diagnosis, guide appropriate management of both the venous thromboembolism and SLE, and ultimately improve long-term outcomes by preventing recurrent thrombosis and complications of untreated autoimmune disease.
.png)