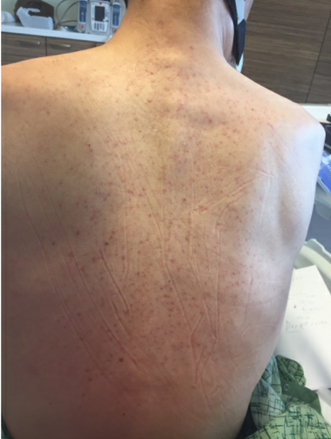
Case Presentation: A 47-year-old man with a history of metastatic colon cancer status post resection and rheumatoid arthritis presented to the emergency department with 4 days of fever, shortness of breath, fatigue and myalgias. He described fevers in a periodic pattern with spikes occurring about 3 times per day. He was found to be tachycardic and hypotensive. Physical exam was also notable for a new petechial rash on his back and chest. Initial labs revealed a lactic acidosis, acute kidney injury, transaminitis, hyponatremia and thrombocytopenia. Chest x-ray demonstrated bilateral interstitial infiltrates. He was fluid resuscitated and treated empirically for suspected septic shock. CT of the abdomen was negative for an intraabdominal source of infection, but incidentally noted a moderate pericardial effusion. Transthoracic echocardiogram re-demonstrated the effusion with hemodynamic compromise, for which a pericardial drain was placed. Culture and cytopathology of the pericardial fluid were unremarkable. Bacterial and fungal blood cultures, urine cultures, AFB smear, Quantiferon Gold, Epstein-Barr viral load, Cytomegalovirus viral load, HIV, COVID-19 and respiratory pathogen PCR panel were all negative. On hospital day 2 the patient developed leukocytosis with bandemia. He was found to have elevated ferritin to 10,724 and C-reactive protein of 14. His rash evolved into a nonpruritic scattered maculopapular rash over the chest and back with faint red macular patches over the bilateral upper arms and thighs (figure 1). He was diagnosed with an acute flare of adult onset Still’s disease. Methylprednisolone was started, with subsequent improvement in his shortness of breath and rash. He was discharged with high-dose Prednisone, which was gradually tapered as an outpatient.
Discussion: Adult onset Still’s disease (AOSD) is a rare systemic inflammatory disorder of unknown pathophysiology. It is generally considered a diagnosis of exclusion, as there is not a pathognomonic physical exam finding or diagnostic laboratory test. However, the diagnosis should be considered in patients who demonstrate the typical constellation of signs and symptoms. AOSD flares are most commonly characterized by recurrent fevers, new rash, sore throat, neutrophilia, elevated inflammatory markers and elevated ferritin levels. The ferritin elevation during an acute flare is rather impressive, usually >3,000, and typically higher than is seen in the setting of infection or malignancy. Other common findings in AOSD flares include polyarthralgia and liver dysfunction. Pericarditis is seen in approximately 30-40% of cases, with cardiac tamponade being a rare and potentially fatal complication. This case illustrates that shock secondary to cardiac tamponade may be the predominant presenting sign of an AOSD flare.
Conclusions: Suspected sepsis is a common condition for which patients are admitted to a Hospital Medicine service and encompasses a wide spectrum of etiologies. While uncommon, adult onset Still’s disease should remain on the differential for patients presenting with fever and shock in the absence of another underlying diagnosis. Other findings suggestive of AOSD include new rash, sore throat, liver dysfunction and significantly elevated ferritin. Recognizing this constellation of findings and diagnosing AOSD is imperative, as the management is different from the treatment of infectious etiologies.