Background: Transitions of patient care are common and vulnerable periods for patient safety. Effective transfer of information from the primary team to the overnight (“cross-covering”) provider has been researched, but less is known about communication from cross-covering providers back to the primary team.
Purpose: The authors aimed to investigate the impact of an electronic health record intervention (a templated dot phrase) on the quality of overnight cross-cover documentation during rapid responses (RRTs) and effect on attending physician notification by internal medicine residents.
Description: The study was conducted at a tertiary-care, university-based institution where significant deficiencies in cross-cover documentation were previously identified. The intervention consisted of a templated dot-phrase in the electronic health record (EHR) for significant clinical events (RRTs) with pre-populated information fields based on a previously developed rubric. After one year of implementation, the authors retrospectively identified patients for whom an RRT activation occurred on internal medicine services and examined the frequency and quality of overnight cross-cover documentation pre- and post-intervention. Secondarily, internal medicine residents were surveyed about perceptions and utilization of the intervention.
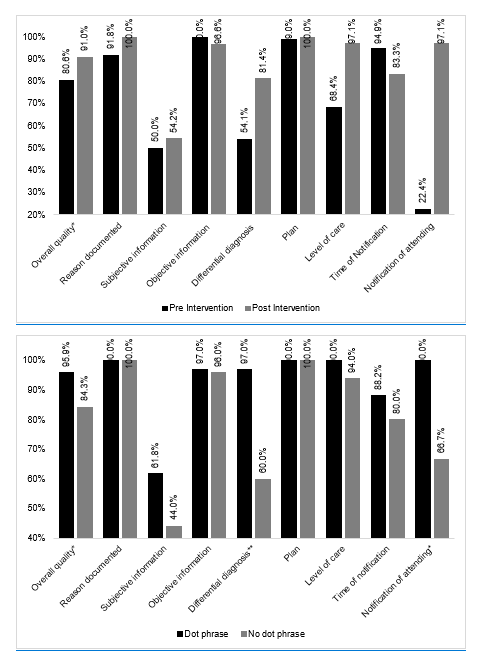
Conclusions: 96 charts were reviewed post-intervention; 62.5% occurred on resident services. The frequency of cross-cover documentation did not change pre- and post-intervention (55.4% vs. 61.5%, p>0.30), however the note quality improved in the post-intervention period (80.6% vs. 91.0%, p<0.001), with significant increase in documentation of differential diagnosis (54.1% vs. 81.4%, p=0.001), and attending physician notification on resident services (22.4 vs. 97.1, p<0.001). Additionally, 50% of residents agreed the intervention helped them to remember to notify the primary attending. This simple EHR intervention improved communication about significant cross-cover events, including enhanced dialogue between residents and attending physicians.