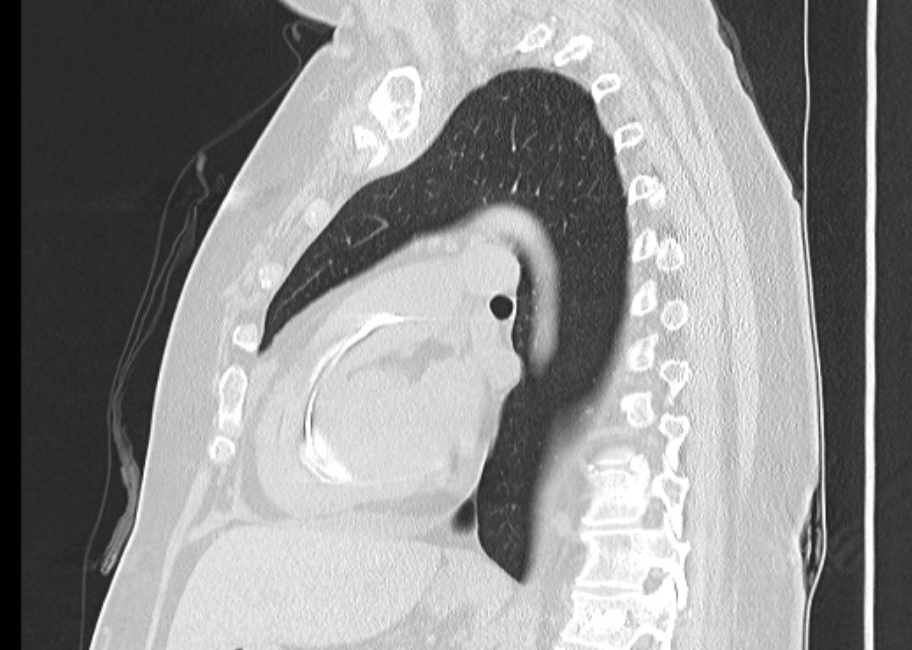
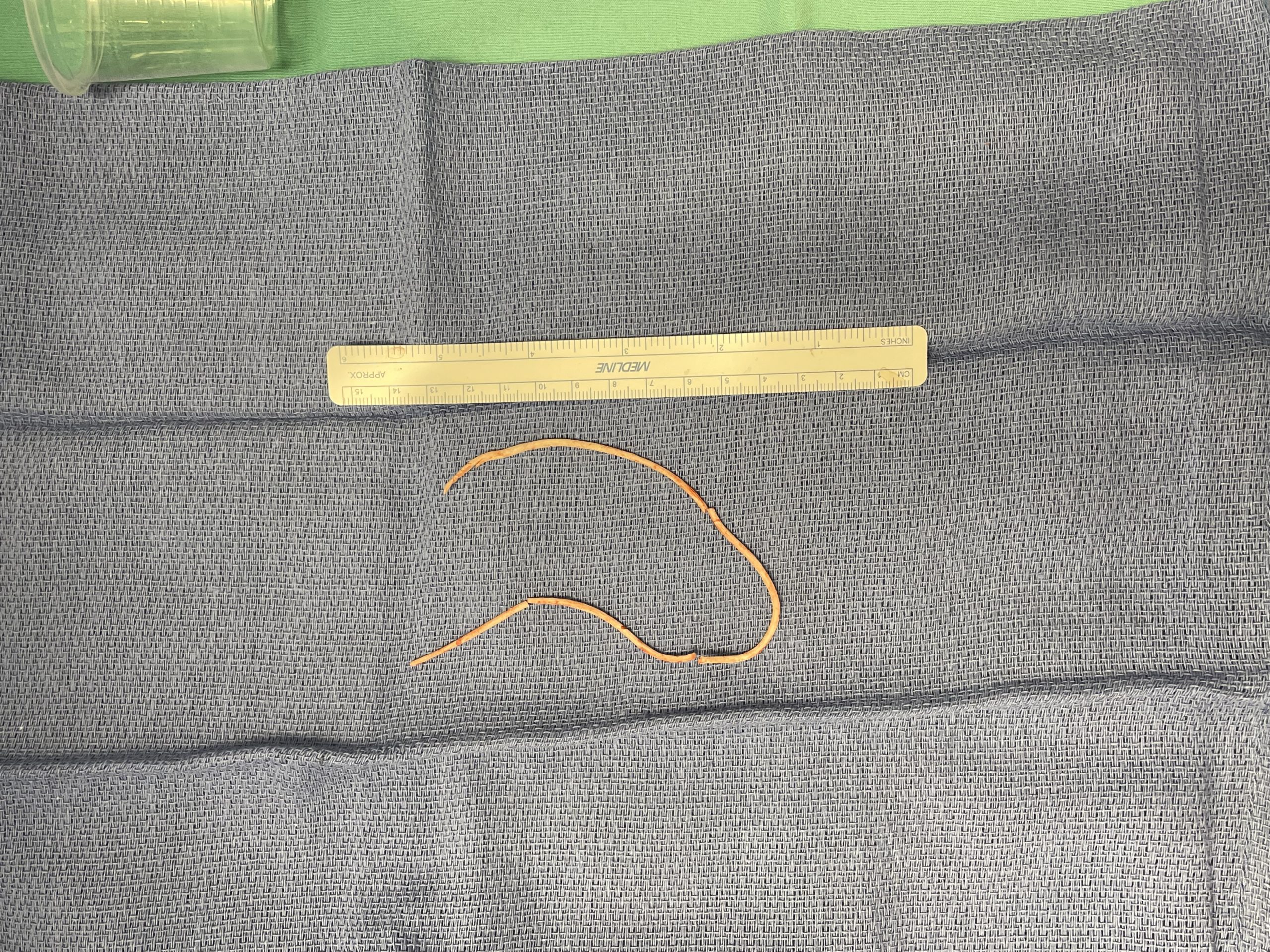
Case Presentation: We present a case of a 55-year-old female who sustained a T12 vertebral fracture from a fall a year and a half ago. She developed worsening pain and subsequently was referred for kyphoplasty. The patient had intense interscapular pain after the procedure combined with dyspnea on exertion. She was evaluated at an outside hospital and diagnosed with an extensive cement embolization of a long, rigid structure that extended from the azygos vein to the superior vena cava, right atrium, right ventricle, and the pulmonary trunk on CT scan. The patient was discharged on Apixaban and presented to St. Joseph’s Hospital for continued symptoms and for a higher level of care. Secondary to the complexity of the case and the risk of cement fracture and distal embolization from a percutaneous IR retrieval, cardiothoracic surgery was consulted. Due to the risks of pulmonary embolization, infection, and damage to cardiac valves from the cement, the patient underwent median sternotomy and cardiac bypass. Four pieces of cement were removed from the heart via dissection of the right atrium and pulmonary trunk. The piece of cement from the azygos vein could not be retrieved and was present on post-operative imaging. Postoperative course was uneventful and the patient recovered well.
Discussion: The kyphoplasty is a relatively new procedure for vertebral compression fractures, now marketed as a minimally invasive treatment. It was first performed in California in 1998. It involves the needle insertion and inflation of a balloon inside the affected vertebrae and the subsequent injection of cement in the space to maintain stability. A retrospective analysis of 102 patients found that 12.7% had cement embolization to varying degrees, so this is not an uncommon phenomenon. There are currently no recommended guidelines for the treatment of such cases, but the literature suggests several cases being treated with anticoagulation for 3-6 months with no surgical intervention. These patients have not been followed regarding further consequences or complications. In severe cases, some patients underwent surgical procedures. Although most patients are asymptomatic, there are reported cases of ventricular perforation, chronic valvular insufficiency, and potential massive pulmonary emboli. Currently, there are very few reported cases of operative embolectomies in such patients.
Conclusions: Cement embolization is a rare but serious complication of Kyphoplasty which can potentially cause side effects ranging from massive pulmonary embolism and valvular insufficiency to life-threatening ventricular perforation. Literature suggests these cases were being treated with anticoagulation for 3-6 months. From our case, we propose that surgical removal is a rational treatment in appropriate patients at institutions where the surgical capabilities are available.