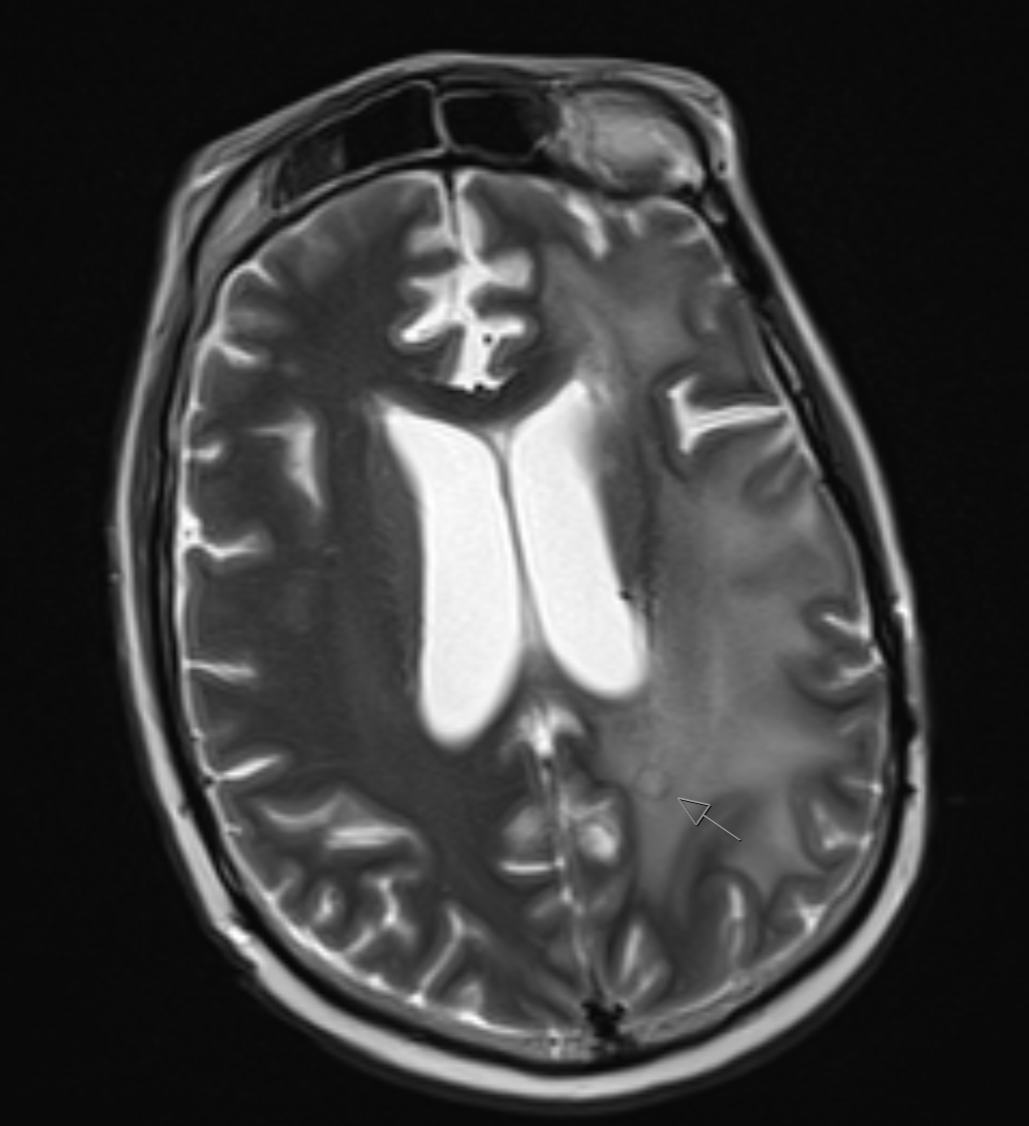
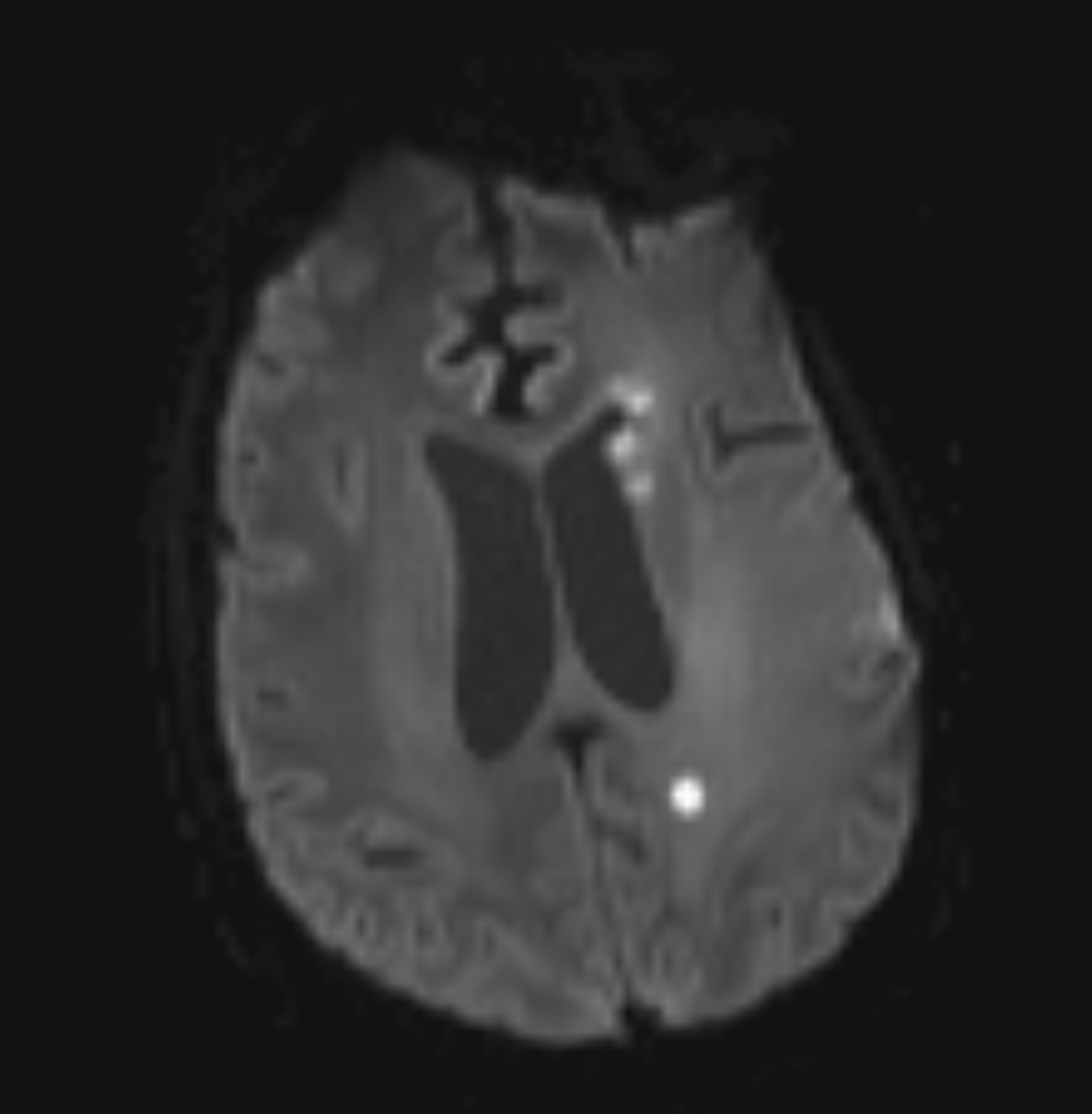
Case Presentation: A 37-year-old female with PMH of high-grade glioma, s/p L frontal craniotomy for tumor resection, with recent diagnosis of leptomeningeal disease, presented to care with several days of altered mental status characterized by cognitive deficits, aphasia, and bilateral leg weakness. One month prior to this presentation, she was evaluated for glioma progression and new leptomeningeal disease. She was treated with corticosteroids, radiation, and bevacizumab and discharged home on tovorafenib without adverse effect prior to presentation. In the ED, she displayed profound lethargy, fatigue and dry cough and was found to be hypoxic, with leukopenia and severe thrombocytopenia. A CT head was unchanged from prior, and a CT chest was notable for acute bilateral pulmonary emboli and RLL necrotizing pneumonia. She was started on anticoagulation and broad-spectrum antibiotics. Blood cultures from admission revealed S. pneumoniae bacteremia for which she was treated with ceftriaxone and azithromycin. Despite antibiotics, her mental status did not improve. Repeat MRI brain was obtained that was significant for possible septic emboli, and lesions displaying a “reverse target sign” that can be seen in cerebral aspergillosis. Lumbar puncture was obtained with findings positive for aspergillosis and active varicella zoster infection. Treatment was expanded to include voriconazole, caspofungin, and acyclovir. She exhibited modest recovery of mental status but still required enteral access for nutrition, which was against her established goals of care. She was transitioned to comfort care and expired.
Discussion: Here we present a case of disseminated aspergillus and VZV encephalitis in a patient with a high-grade glioma presenting with altered mental status. Her symptoms were initially attributed to her progression of glioma-related disease. There were no obvious exposures to either VZV or aspergillus, and her glioma treatment regimen was not expected to be high-risk for opportunistic infection compared with other chemotherapy regimens. The true nature of her infection was only revealed through pathognomonic imaging findings. This serves as a reminder to maintain an open differential for altered mental status and to avoid anchoring bias towards suspicious past medical history, while considering relative immunocompromised status. Additionally, it highlights the benefit of advanced and serial imaging in differentiating disease etiology.
Conclusions: In conclusion, it is imperative that clinicians maintain a broad differential when evaluating a patient presenting with altered mental status—particularly in cases of glioma or other intracranial malignancies. Chronic steroid use and immunotherapy can leave such patients susceptible to opportunistic infections. The glioma diagnosis can cloud differential diagnosis and lead to anchoring bias. Close collaboration with a patient’s family and their long-term outpatient provider can provide important collateral in determining potential etiology and the need for additional testing.