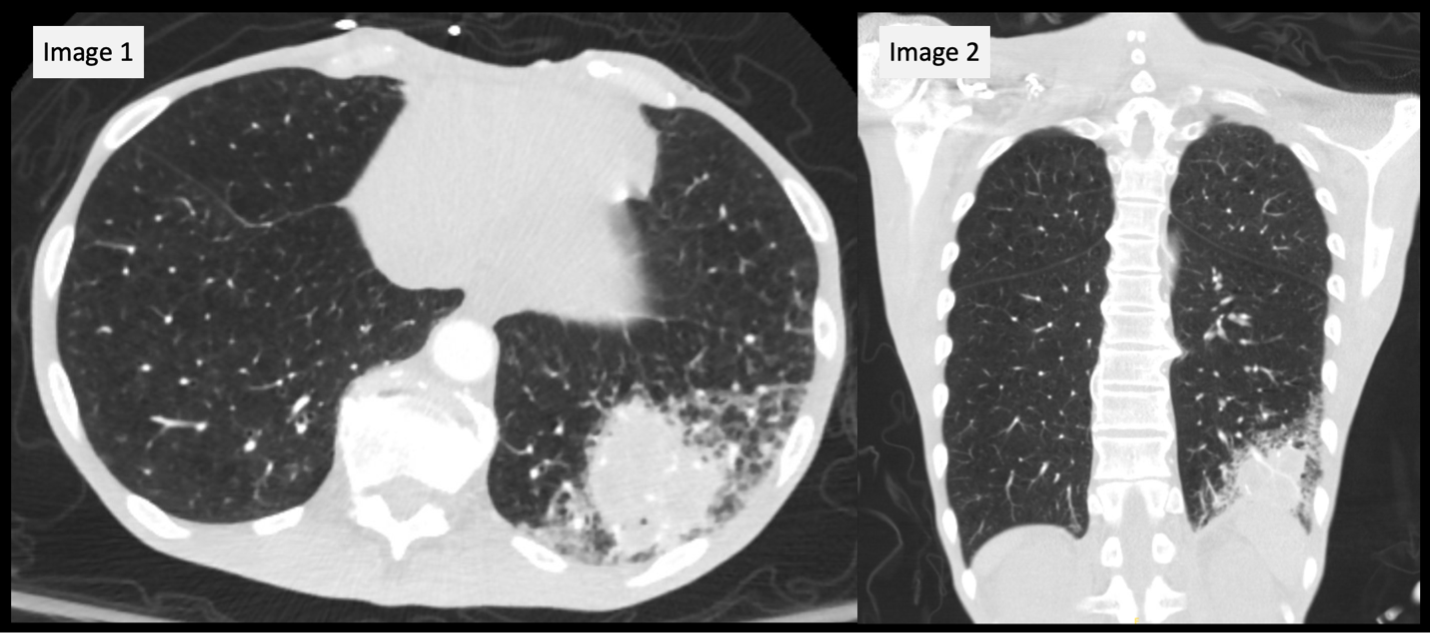
Case Presentation: A 54-year-old man with neurofibromatosis and recent tracheostomy and gastrostomy for newly diagnosed hypopharyngeal squamous cell carcinoma presented with two weeks of worsening cough, increased tracheal secretions with brown sputum and progressive shortness of breath now occurring at rest. He appeared cachectic. He was hypotensive and tachycardic. Physical examination revealed brown tracheostomy secretions, diffuse rhonchi and a tender enlarging erythematous lesion in the left lower chest wall amongst the multitude of neurofibromas present. CT chest revealed a 5 cm pleural based left lower lobe mass-like lesion concerning for malignancy, abscess or necrotizing infection (Figure 1). Broad spectrum antimicrobials were initiated for presumed sepsis secondary to pneumonia. The cutaneous lesion, which initially appeared quite similar to his surrounding neurofibromas evolved into a more fluctuant mass that was drained and cultured. Although chest imaging suggested possible metastatic spread, additional CT staging demonstrated local malignancy progression without other signs of distant metastatic disease. He was discharged on oral antibiotics after symptomatic improvement. A week later, the culture from the drained abscess grew Actinomyces radingae leading to initiation of targeted therapy.
Discussion: Thoracopulmonary actinomycosis is an uncommon and often deceptive infection that closely resembles malignancy, chronic pneumonia or fungal/nocardial abscesses [1]. Thoracopulmonary actinomycosis comprises only a minority of the cases and often presents with weight loss, chest wall involvement and a mass-like lesion that is often interpreted as malignancy on imaging [2]. This patient’s profound cachexia, recent diagnosis of head and neck squamous cell carcinoma, and tracheostomy tube placement led to a diagnostic dilemma that favored malignancy progression or an aspiration-related infection. Actinomyces species are slow growing and often missed in patients who previously received antibiotics [3]. In this case, identification occurred only after a full week of incubation of the drainage collected from the soft tissue abscess. Actinomyces radingae is a rare species most often associated with cutaneous or breast infections which makes its presence in this clinical context particularly challenging [4-6]. The case highlights the importance of maintaining diagnostic vigilance when radiographic and clinical features point toward both infection and malignancy especially in patients with structural airway alterations or recent instrumentation.
Conclusions: Thoracopulmonary actinomycosis may closely resemble metastatic cancer and bacterial pneumonia leading to delays in proper diagnosis, especially in medically complex patients. It requires a high index of suspicion coupled with tissue sampling or drainage of abscesses. Early recognition is paramount in the avoidance of misclassifying a treatable infection as malignant progression and to ensure that appropriate antimicrobial therapy is initiated in a timely manner.