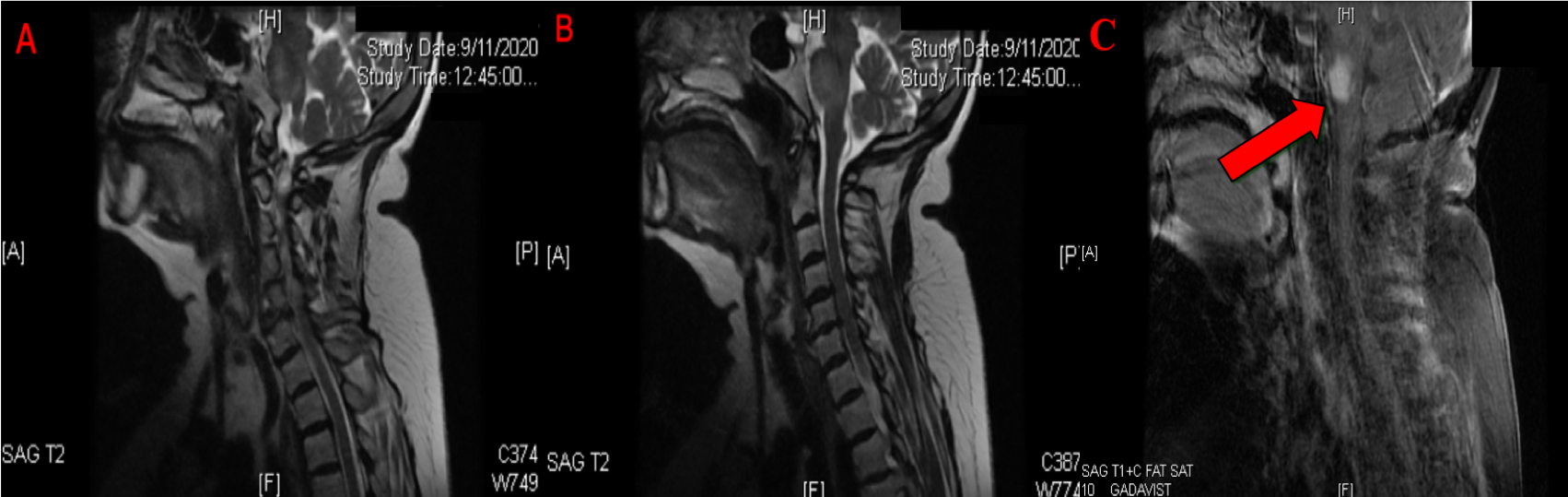
Case Presentation: A 73 year old female presented with acute onset of recurrent falls lasting for 1 week. On day 2 of her hospitalization, hematuria with dysuria was present, which was treated as an UTI. Physical examination revealed progressive ascending weakness from lower to upper extremities with decreased reflexes bilaterally. She also developed urinary retention progressively with a residual volume of more than 200 cc. Given her clinical symptoms, Guillain-Barré syndrome (GBS) was suspected. A lumbar puncture indicated the presence of albuminocytologic dissociation with an elevated protein of 84 mg/dL and normal WBC count. Her results were followed up with an MRI of the c-spine that illustrated abnormal signal intensity and enhancement of the pons suggesting a demyelinating process consistent with Miller Fisher Syndrome (MFS). She did not have any fluctuating blood pressure or bulbar abnormalities but did, however, experience marked dysarthria. She was started on IVIG and received 7 doses in 2 days with supportive care.
Discussion: MFS is a rare demyelination variant of GBS characterized by paralysis of ocular muscles, abnormal muscle coordination and decreased/absent reflexes. Hospitalists need to start treatment in a timely manner especially when signs of brainstem involvement are present in order to prevent further complications. In MFS, a focal inflammatory reaction is responsible for attacking the myelin producing Schwann cells or peripheral nerves. Macrophages and lymphocytes are responsible for mounting this attack against the peripheral nervous system. The guidelines for treatment of MFS involve IVIG, plasmapheresis and supportive care. MFS is a self limiting benign condition in which patients are expected to recover within 6 months of disease onset in most cases. For those experiencing ataxia, like the patient presented in this case vignette, these symptoms are expected to resolve within 3-4 months. According to a clinical trial performed in 20 patients who suffered from severe fatigue as a complication of GBS, 16 of these subjects were established to make relatively good recovery during a twelve weeks bicycle extensive training program.
Conclusions: The patient in this case vignette initially presented with ascending paralysis consistent with GBS. The unique aspect of this case is the involvement of the pons on the T2 weighted imaging of MRI. Unconventional findings that require further research are the brainstem involvement. In this atypical presentation of MFS, central nervous demyelinating processes provide a hybrid pathology that blurs the conventional lines between central versus peripheral demyelinating disorders. It is important for hospitalists to be aware of this atypical presentation so that treatment with IVIG can be started early in the disease process.