Case Presentation: A 72-year-old man with extensive-stage small cell lung carcinoma was admitted for observation following his first infusion of tarlatamab-dlle (Imdelltra), a bispecific T-cell engager (BiTE) targeting DLL3. His medical history included chronic obstructive pulmonary disease with chronic hypoxic respiratory failure and hypertension. He remained stable during 24 hours of inpatient monitoring and was discharged. Within 24 hours, he returned with profound weakness, low-grade fever, chills, and increased oxygen requirements. His blood pressure declined from 133/86 mmHg to 82/53 mmHg within one hour, heart rate was 120 bpm, and temperature 100.2°F. He appeared acutely ill and mildly disoriented. Laboratory results revealed leukocytosis (WBC 16.98 × 10⁹/L), hyponatremia, and elevated lactate (7 mmol/L). Urinalysis, chest radiography, and a respiratory viral panel were negative. Despite fluid resuscitation and empiric broad-spectrum antibiotics for presumed sepsis, his condition worsened. Review of oncology documentation identified recent BiTE therapy, raising strong concern for CRS. Tocilizumab and dexamethasone were administered after consultation with oncology, leading to rapid improvement in hemodynamics and mental status. Blood and urine cultures remained negative, and the patient was discharged in stable condition after 48 hours.
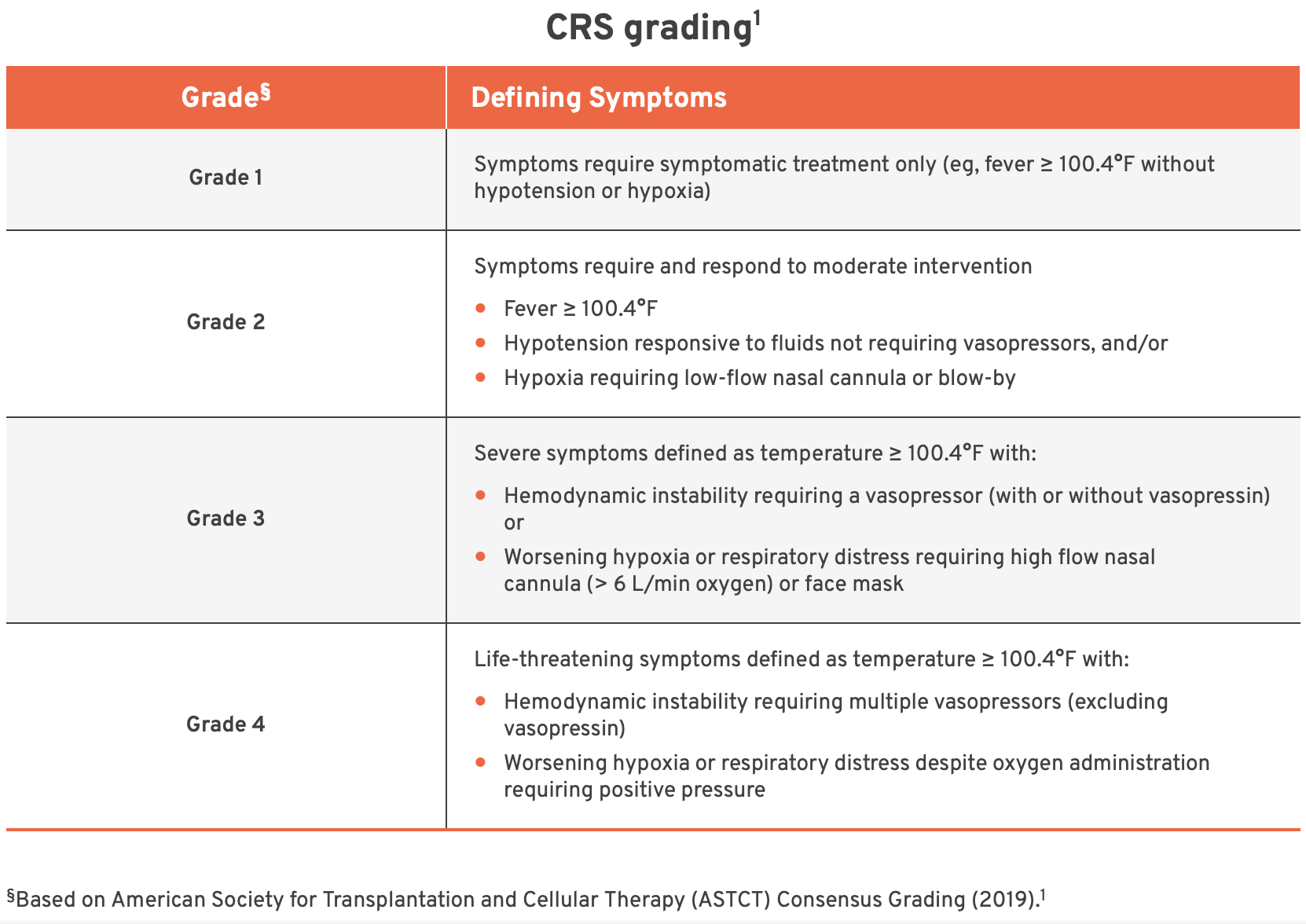
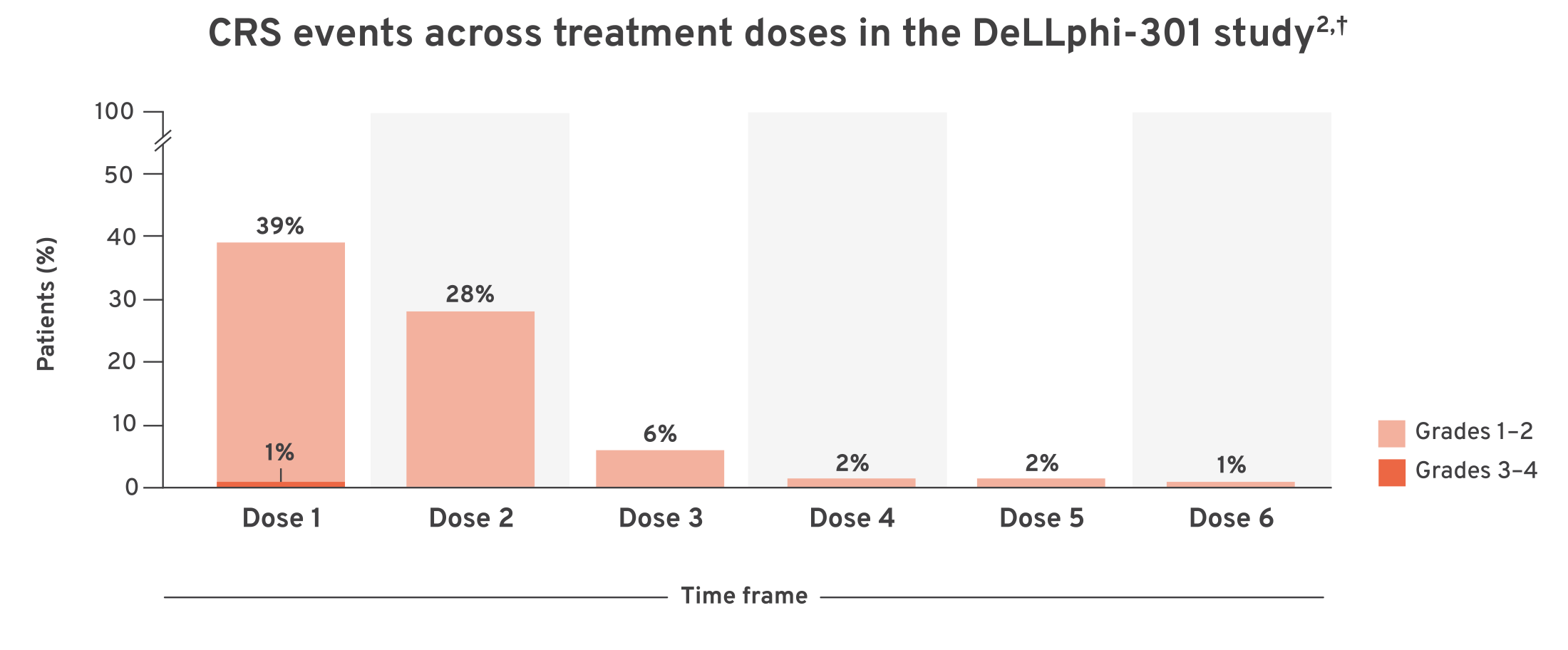
Discussion: Cytokine release syndrome (CRS) is a potentially life-threatening systemic inflammatory response resulting from excessive cytokine activation. It may lead to multiorgan dysfunction and is often clinically indistinguishable from sepsis without a high index of suspicion. As the use of immune effector cell therapies expands, hospitalists are increasingly likely to encounter this entity.CRS represents a distinct clinicopathologic process from the broader “cytokine storm” and is now well recognized with immunotherapeutic agents such as CAR-T cells, BiTEs, and immune checkpoint inhibitors. The reported incidence of CRS with Imdelltra is approximately 55%, typically within 13 hours of infusion. This case was notable for delayed onset following discharge, underscoring that CRS can manifest beyond standard monitoring periods and closely mimic sepsis—a frequent diagnostic pitfall. CRS is graded using American Society for Transplantation and Cellular Therapy (ASTCT) criteria, which guide therapeutic interventions. Although this patient met criteria for Grade 2 CRS, early initiation of tocilizumab and corticosteroids was warranted given his rapid deterioration, with prompt clinical recovery thereafter.
Conclusions: Hospitalists should maintain a high index of suspicion for CRS in patients presenting with sepsis-like syndromes following recent immunotherapy. Early recognition and timely initiation of immunomodulatory therapy are essential to optimize outcomes, prevent organ failure, and reduce unnecessary antimicrobial exposure.