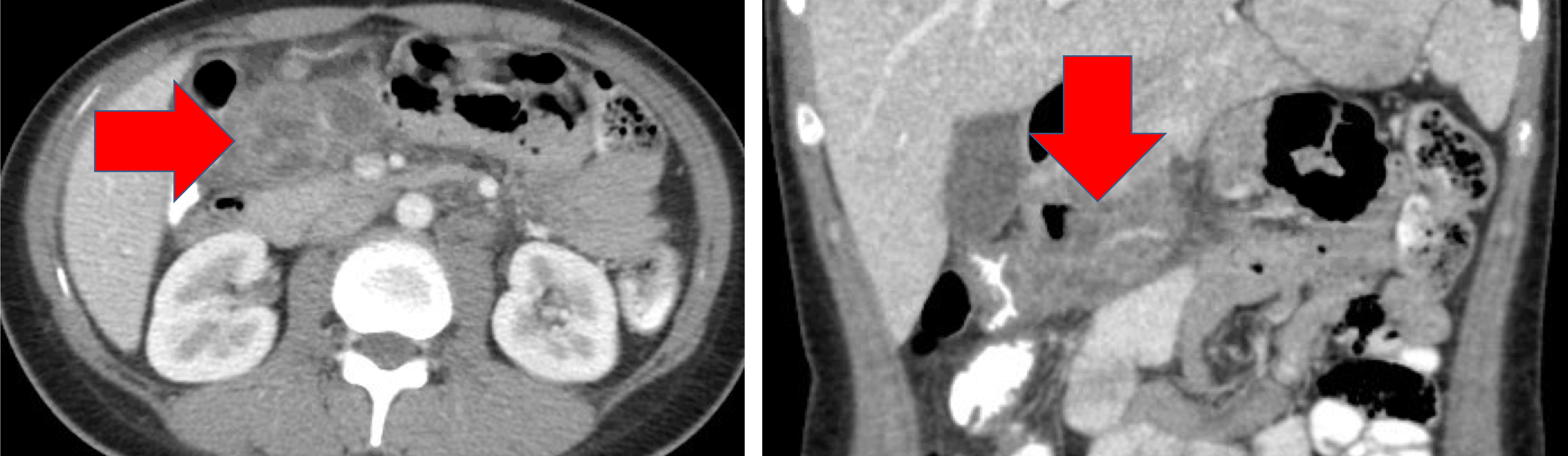
Case Presentation: A 23-year-old woman from Vietnam with no known past medical history presented to her primary care physician due to an abdominal mass. She first noticed the mass one month prior to presentation. It was associated with abdominal bloating and worsening sharp abdominal pain as well as a five-pound weight loss and decreased appetite. Her primary care physician referred her for further work-up with a surgical oncologist. CT of the abdomen demonstrated a 7×5 cm mass near the pancreatic head with solid and cystic components. Several days before her surgical oncology visit, she presented to the ED with fevers, chills, and night sweats. Repeat CT abdomen was unchanged. She had an intermittent dry cough since childhood. When she was two, her father was diagnosed with tuberculosis (TB) after biopsy of a neck lump. She tested negative for TB at that time. Two years prior to presentation she had a borderline PPD without follow-up, and one year prior she had a poorly administered PPD with a normal chest x-ray. She visited Vietnam one year prior.Her surgical oncologist ordered a Quantiferon gold, which resulted positive. Upon returning one week later for her CT-guided biopsy, she was admitted due to concern for TB. Before biopsy, her physical exam was significant for a firm, clementine-sized mass in her mid-abdomen. Her exam on admission was notable for tenderness at her biopsy site with deep palpation limited by pain; her pulmonary exam was unremarkable. Pathology of the mass revealed severe acute and chronic inflammation. AFB stain was negative; however, TB-PCR of abdominal fluid was positive. CT chest revealed sub-centimeter scattered bilateral pulmonary nodules. She had three negative AFB sputum smears and negative sputum TB-PCR. Sputum AFB culture grew acid fast bacilli. She was counseled on RIPE therapy and was discharged to initiate TB treatment with her county health department.
Discussion: The differential diagnosis for this patient with an abdominal mass and subacute night sweats, decreased appetite and weight loss included lymphoma, carcinoma of the colon or small bowel, germ cell tumor or other ovarian tumor, hepatic abscess and TB. Workup for abdominal masses should include a detailed history, physical, basic lab studies including pregnancy test and imaging studies. Further testing with tumor markers or endoscopy can be considered depending on initial workup. Biopsy was indicated in this patient to determine if the mass was malignant or benign. Disseminated TB, defined as having two or more non-contiguous sites of infection, lacks the typical diagnostic and imaging findings of pulmonary TB. Extra-pulmonary manifestations are present in one in five individuals diagnosed with TB. The patient’s past TB exposure and country of origin were key to the diagnosis. While tissue pathology is diagnostic of malignancy, the classic histologic findings of TB are present in less than one-third of cases. PCR is the most specific and sensitive diagnostic tool for TB, especially in peritoneal fluid.
Conclusions: TB should be included on the differential for patients with a wide variety of presenting symptoms. Exposure histories and characteristic symptomatology in atypical presentations are key elements of history that can lead to diagnosis.