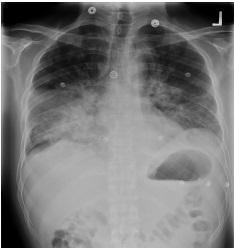
Case Presentation: A 30 year-old MSM with a newly diagnosed HIV presented with shortness of breath and cough. He stated that he became sick 5 weeks ago at which point he made an appointment to see his PMD where he was diagnosed with RML pneumonia and was given 5 day course of oral antibiotics. He had also developed multiple small bruise-like lesions on his bilateral lower extremities over the past few months, with several appearing over the last 2-3 weeks. Due to the persistent symptoms with hypoxemia, he was sent to the emergency room where he was found to have extensive bilateral pulmonary nodules, axillary and inguinal adenopathy, RML opacification along with bilateral pleural effusions. On admission, he was hypoxemic at 96% on 2L NC and tachycardic at 115 bpm. His labs were significant for CD4 T-cell count of 4/mm3, positive AFB culture from bronchoscopy and sputums, likely MAC, positive viral culture and low level positive PCR for CMV. With several subsequent biopsies, he was diagnosed with widespread Kaposi Sarcoma (KS) with cutaneous, pulmonary and lymph node involvement with extension into retroperitoneum. He was started on HAART after tuberculosis was ruled out. As he clinically improved after the regimen with dramatic improvement in HIV viral load from 94,010 copies/mL to 118 copies/mL in 2 weeks, he was planned for chemotherapy. Yet, he subsequently had multiple re-admissions for worsening SOB and new lesions on his penis and tongue, both of which were clinically diagnosed as KS. He quickly deteriorated into acute respiratory failure and subsequently into bradycardia and PEA arrest.
Discussion: The prevalence of AIDS-related KS has markedly decreased after introduction of HAART although it remains one of the most common AIDS-defining malignancies, accounting for severe morbidity and mortality. Despite efforts to diagnose HIV infection early, a substantial number of patients still present late with CD4 T-cell count < 200/mm3, increasing risk for IRIS: it is defined as a worsening of a patient’s clinical condition after initiating HAART, attributable to the recovery of the immune response to viable or nonviable pathogens. Multivariate analysis identified four independent predictors of KS-associated IRIS: clinical KS at the pre-HAART visit, detectable pre-HAART plasma KS herpesvirus DNA (KSHV or HHV-8), hematocrit <30% and pre-HAART plasma HIV-1 RNA levels. Our patient had clinical manifestation of IRIS-KS with increased number of KS skin lesions and a change in consistency or ulceration, lymphedema, involvement of mucosa other than the oral mucosa.
Conclusions: Here, we presents a fatal case of AIDS-related KS. It is important for the internists to recognize the diagnosis as it is associated with high mortality. No randomized controlled trials have established the best timing for starting HAART in patients with KS, although uncontrolled data suggest that early initiation may be beneficial.