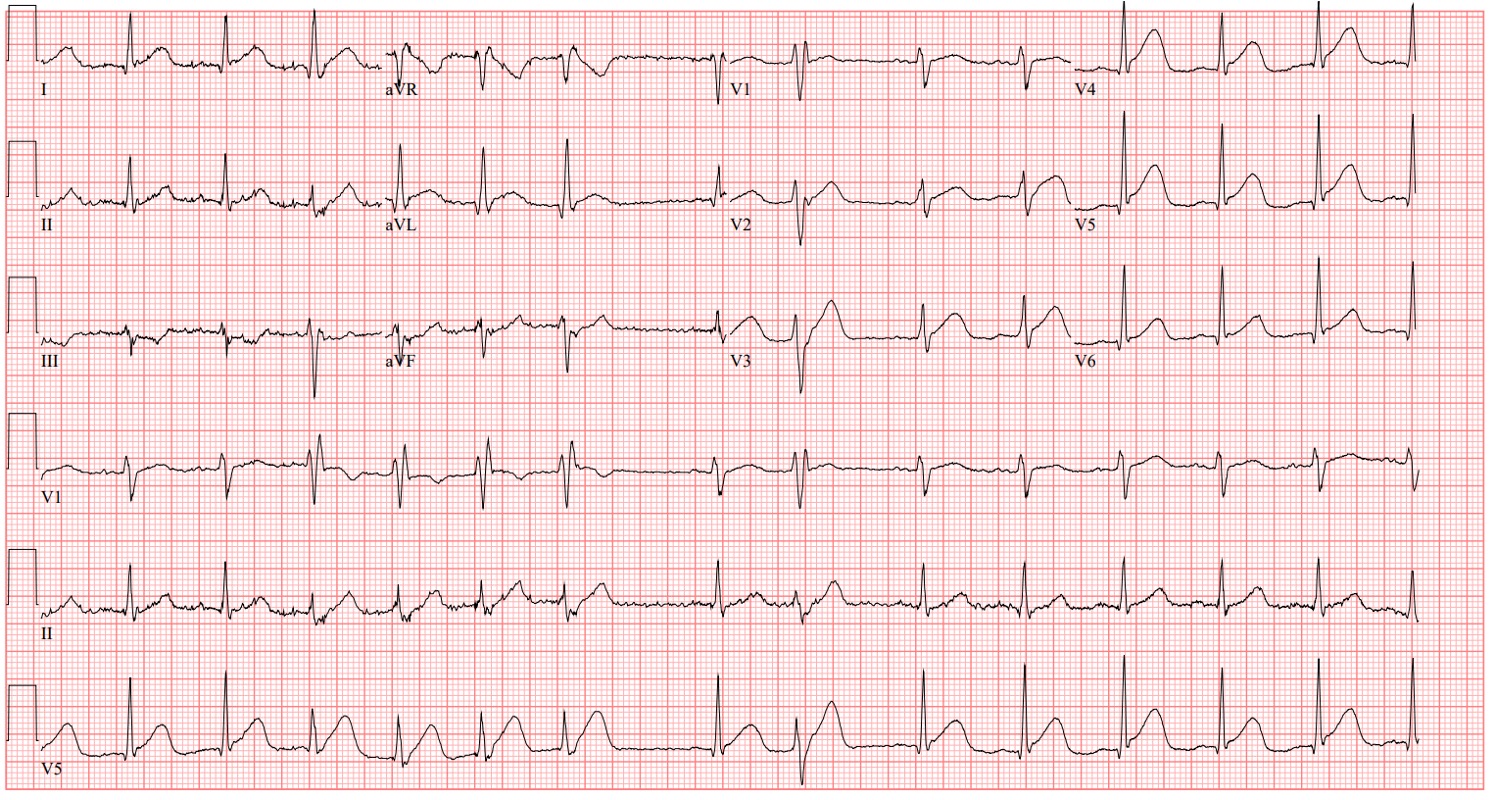
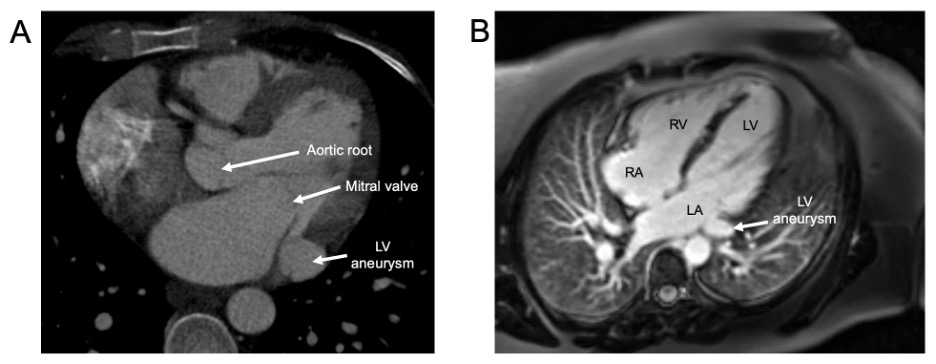
Case Presentation: A 27-year-old G6P4 female at 28 weeks of gestation presented with fever, headache, myalgias, nausea, vomiting, and diarrhea. Medical history was significant for polysubstance use, hepatitis C, anxiety, and depression. On the evening of presentation, she reported new-onset central chest pain. Vitals were significant for rectal temperature 93 F, blood pressure 95/58, and heart rate 94 bpm. Electrocardiography showed ST-segment elevation in the anterolateral leads (Figure 1). High sensitivity troponin was 106 ng/L with peak of 33,704 ng/L. An emergent coronary angiogram revealed a Type 1 spontaneous coronary artery dissection (SCAD) of the left main coronary artery, extending down the left anterior descending artery and left circumflex artery, with total occlusion of the ramus. Echocardiography showed ejection fraction (EF) of 40%, global hypokinesis of the anterior segments, and mitral valve posterior leaflet pathology causing moderate, eccentrically directed regurgitation. Conservative management was elected, including daily aspirin and titration of metoprolol.Hospitalization was complicated by prolonged MSSA bacteremia and tricuspid valve endocarditis requiring a 6-week course of intravenous oxacillin. At 34 weeks, fetal monitoring showed decelerations with abnormal biophysical profile prompting urgent caesarean section. Postpartum echocardiography showed EF 40% and mildly enlarged LA with aneurysmal segment along the posterior leaflet of the mitral valve. Transesophageal echocardiogram was pursued to further characterize the lesion, showing an outpouching posterior and superior to the mitral annulus and LV-LA communication (physiology similar to mitral regurgitation but around the mitral valve). Cardiac MRI revealed mild LV dilation, LA outpouching, and subendocardial fibrosis with non-viable segments in the LAD distribution (Figure 2).Two months into admission, she underwent CABG (LIMA-diagonal branch; SVG-OM), mechanical mitral valve replacement, and repair of the LV pseudoaneurysm. Intraoperatively, the pseudoaneurysm was found to extend from the LV into the LA through a posterior fistulous tract. She was also found to have a very small, dissected LAD and dissected high diagonal branch, confirming the P-SCAD diagnosis.
Discussion: Pregnancy-associated SCAD is a rare condition that can be easily missed, leading to life-threatening complications for mother and fetus [1]. Peripartum patients are at high risk due to hormonal changes resulting in impairment of collagen synthesis and elastic fiber makeup of the tunica media [2]. In combination with other risk factors, such as intravenous drug use, these patients may experience overwhelming hemodynamic consequences [3, 4]. In this case, we suspect SCAD developed from the dual arterial insults of pregnancy and chronic cocaine/amphetamine use. This case of SCAD is especially unique as it illustrates multivalvular involvement with a peculiar complication of LV pseudoaneurysm and LV-LA communication proximal to the mitral annulus requiring surgical repair.
Conclusions: Herein, we describe a complex case of P-SCAD with multiple cardiac complications in a pregnant patient. This case required excellent coordination of interdisciplinary teams, including cardio-obstetrics, cardiac surgery, and addiction specialists. To our knowledge, there have been no case reports describing antepartum SCAD complicated by endocarditis, LV pseudoaneurysm, and LV-LA communication.