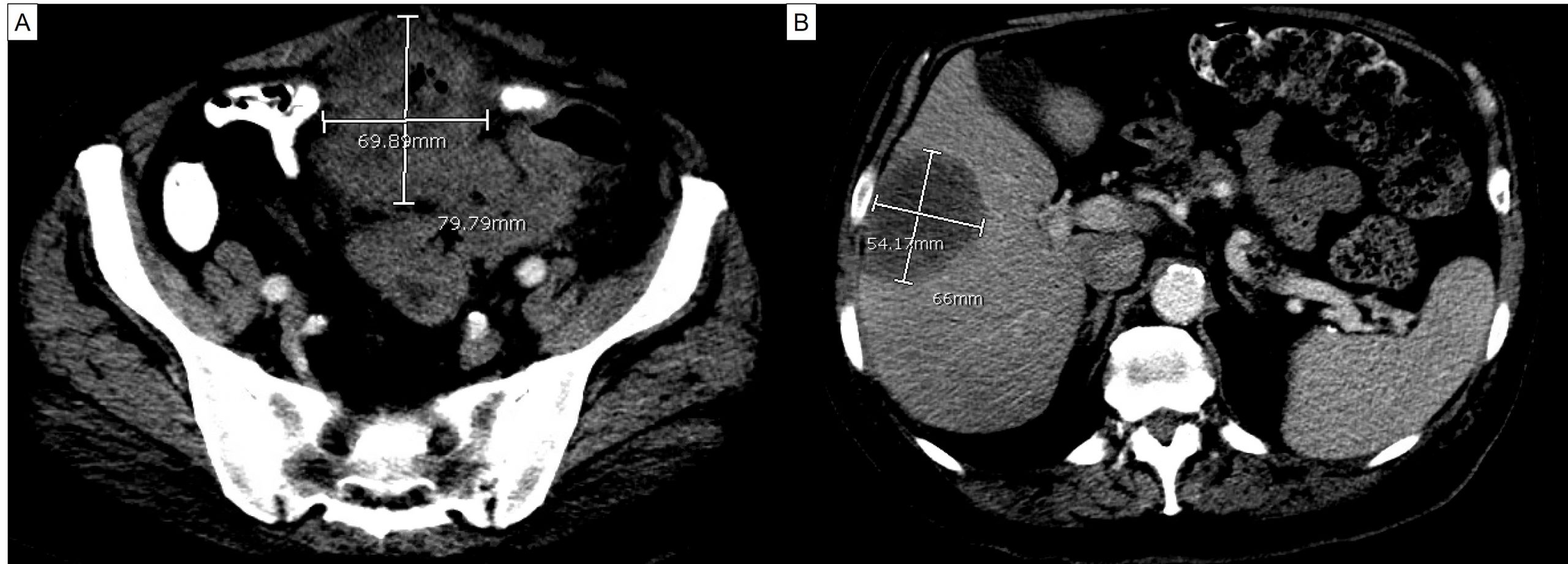
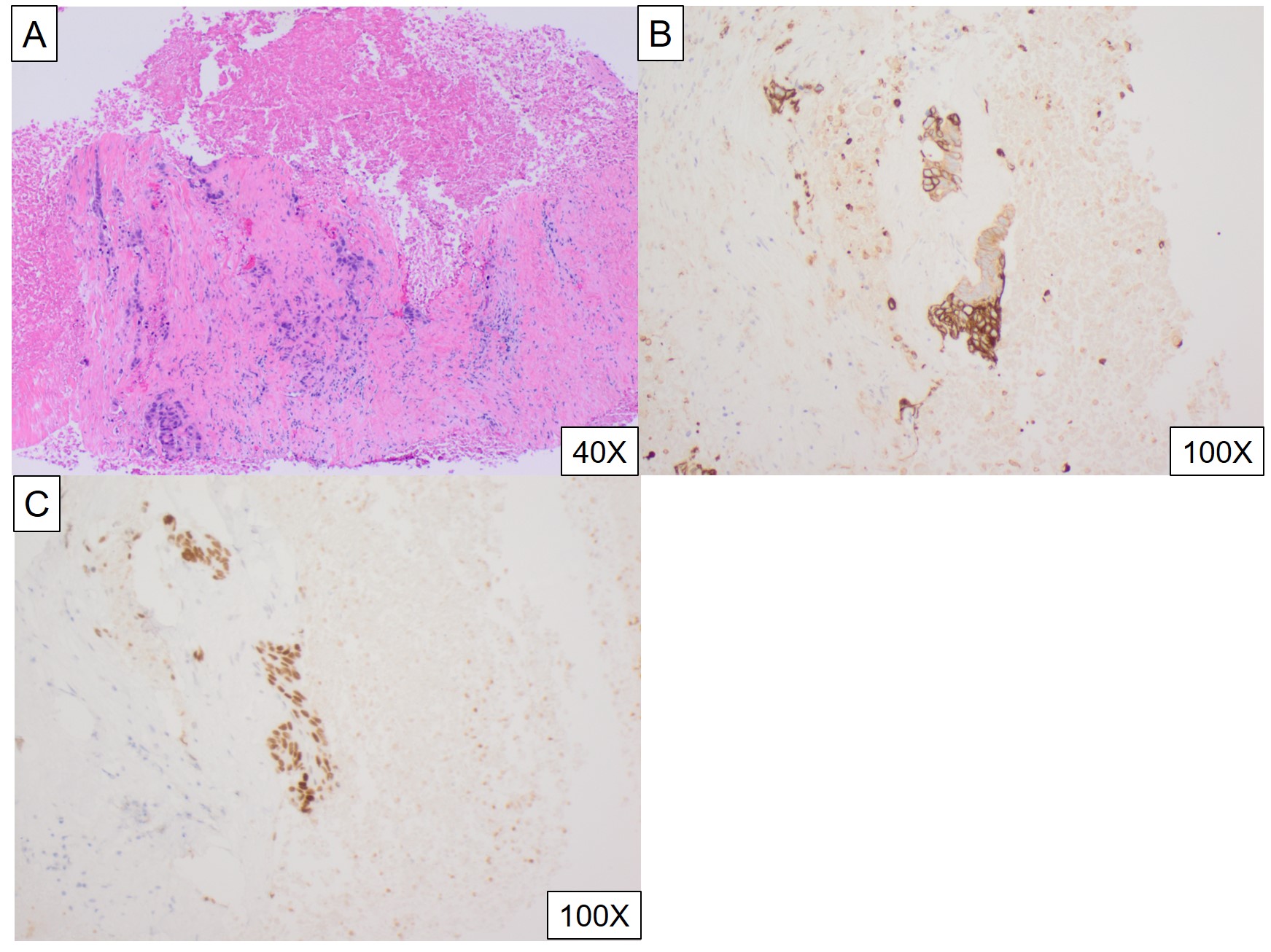
Case Presentation: A 71-year-old man presented with pus from the umbilicus. Past medical history was pertinent for persistent urinary tract infection for a month, complicated by feculent urine and pneumaturia despite two rounds of antibiotics, and 20-lb weight loss. He was found to have purulent drainage from the umbilicus. Lower abdomen was tender without rebound or guarding. Rectal exam was normal, without fistula visualized. CT scan revealed a large abscess extending from the umbilicus to the anterior urinary bladder with multiple locules of gas. There was also an accidental finding of low-density lesion of the right lobe of the liver, 5.4 X 6.6 X 7.2 cm. The patient underwent surgical incision of the intra-abdominal abscess and CT-guided liver lesion drainage and biopsy. Initial biopsy only revealed necrotic tissue. The purulent drainage from the umbilicus recurred 4 months after the operation. Repeat CT scan revealed extensive necrotic changes from the umbilicus to the urinary bladder, which was along the expected course of the urachus, and the right lobe liver mass similar to the prior study. The patient underwent repeat CT-guided liver mass drainage and biopsy. It showed adenocarcinoma in the background of marked necrosis. Immunohistochemical (IC) staining was positive for CDX2 and CK20, and negative for CK7, GATA-3, HepPar-1 and NKX3.1. This was consistent with urachal adenocarcinoma with liver metastasis. The patient was started on FOLFOX (Folinic acid (leucovorin), Fluorouracil (5-FU), Oxaliplatin (Eloxatin)). Repeat CT scan 2 months after the initiation of the therapy demonstrated partial response.
Discussion: The urachus is a remnant structure from the allantois. It connects the dome of the urinary bladder to the umbilicus without any physiological function. Urachal cancer is extremely rare and only accounts for less than 1% of all bladder cancers. There have been case reports and series documenting this uncommon cancer. The most common symptoms are urinary symptoms such as dysuria, hematuria, abdominal or pelvic pain. Diagnostic criteria for urachal cancer are: (1) location of the tumor in the urinary bladder dome or anterior wall; (2) epicenter of carcinoma in the bladder wall; (3) absence of widespread cystitis cystica or cystitis glandularis beyond the dome and anterior wall; (4) absence of a known primary malignancy elsewhere. The initial image study of our case clearly met most of the aforementioned criteria. The repeat liver biopsy was necessary to confirm the origin of primary cancer. The IC results of urachal adenocarcinoma is generally positive for CDX2 and CK20. In our case, besides characteristic urachal adenocarcinoma IC findings, the negative HepPar-1 and NKX3.1staining made liver and prostate origin malignancies less likely. There is also lack of vesicle or colonic origin lesion identified in this case. Nonmetastatic diseases are usually managed with resection. There is no clear recommendation of chemotherapy choice. Several previous metastatic cases showed variable success with colorectal cancer regimen such as FOLFOX or FOLFIRI (Irinotecan, Fluorouracil (5-FU), Folinic acid (leucovorin)).
Conclusions: Urachal cancer should be considered with persistent urinary symptoms and abdominal pain. Treatment modalities for colorectal cancer can be used for urachal cancer.