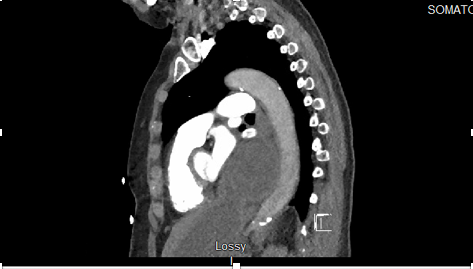
Case Presentation: Introduction:Hiatal Hernia is a common condition. Hiatal hernias rarely cause cardiac symptoms such as dyspnea and chest pain. Here we present an extremely rare case of a giant hiatal hernia causing typical chest pain and actual ST-segment elevations in inferior leads of EKG. Case ReportThis is a case of 76-year-old female who presented to the emergency department with complaints of midsternal chest pressure with radiation into the neck. Her EKG showed ST-segment elevations prominent in inferior leads, initial troponin was within normal limits. She was taken to the cardiac catheterization lab for further evaluation and treatment. She was found to have no major coronary blockages. There was some potential wall motion abnormality in the inferior wall which could account for the ST changes and suspicion for stress-induced cardiomyopathy. 2D echocardiogram showed compression of the posterior wall of the left atrium. This prompted a CT Chest with contrast which showed large hiatal hernia compressing the heart posteriorly.
Discussion: Hiatal hernias are usually asymptomatic but can manifest with nonspecific abdominal symptoms, exercise intolerance, and dyspnea. Rarely, gastric volvulus, hemorrhage, and respiratory distress may occur. Impingement of the left atrium, pulmonary veins, and coronary sinus can result in reduced cardiac output. A key diagnostic clue is postprandial syncope resulting from a decrease in left atrial volumes after meals. Although, our patient did not manifest it. While mechanical compression is likely to be the main mechanism of cardiac presentations, gastroesophageal reflux may also cause the release of local and systemic cytokines and thus result in heat and myocardial inflammation. Additionally, there may be associated with sympathetic nerve and vagal nerve stimulation through either local heat or compression. More studies are required to better understand the mechanism. Atrial arrhythmias have also been described, which are likely attributable to left atrial compression. A large observational study demonstrated that there is a higher prevalence of atrial fibrillation at all ages with hiatal hernia compared to the general population. Surgical repair of large hiatal hernia has been proven to significantly relieve symptoms. However, recurrence has been documented and long-term follow-up should be considered.
Conclusions: Each year over 6 million Americans present to the emergency department with complaint of chest discomfort. Of those only 20‐25% eventually receive the diagnosis of acute coronary syndrome. This case highlights the importance of maintaining a high index of suspicion of a large hiatal hernia as a rare cause of cardiac compression in a patient with chest pain.