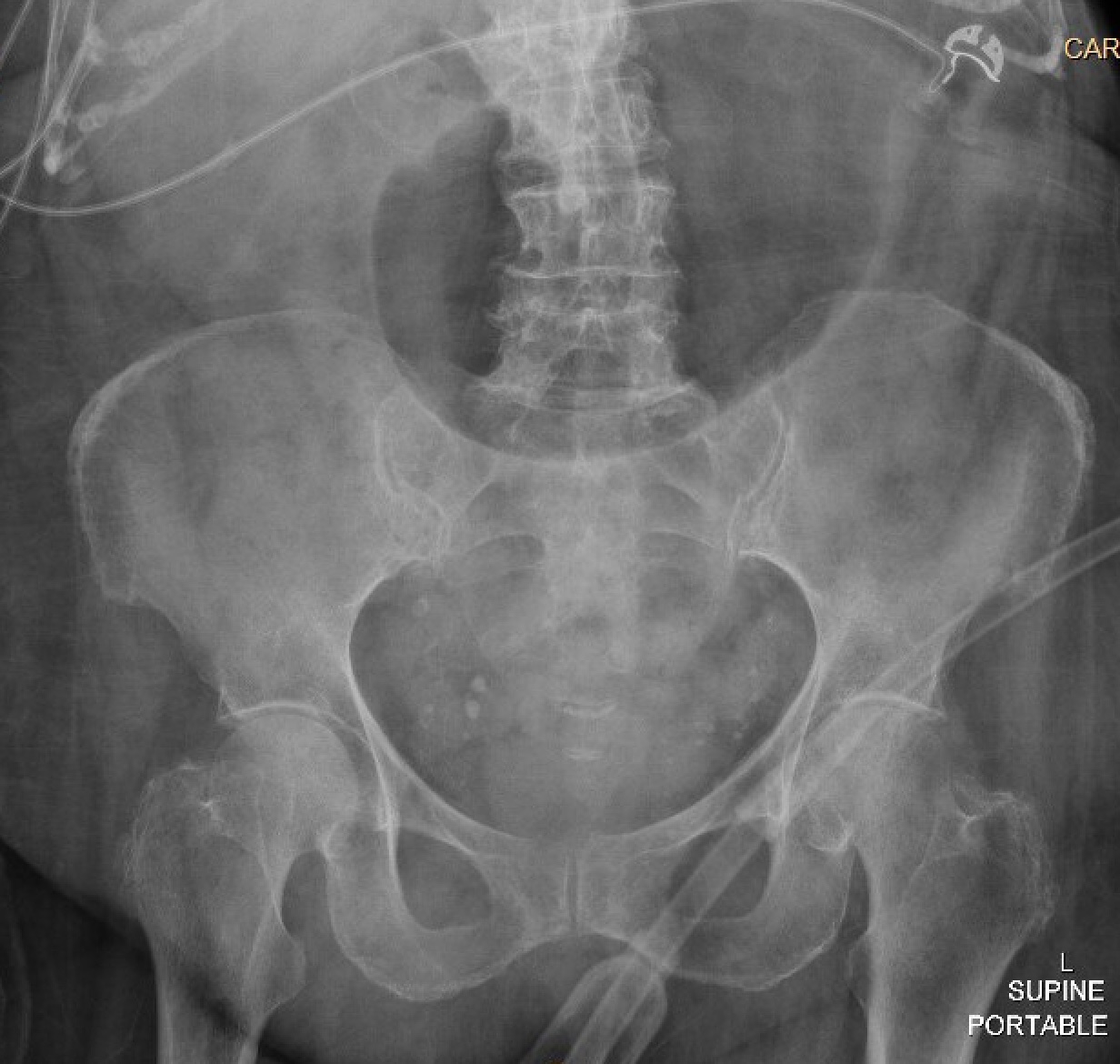
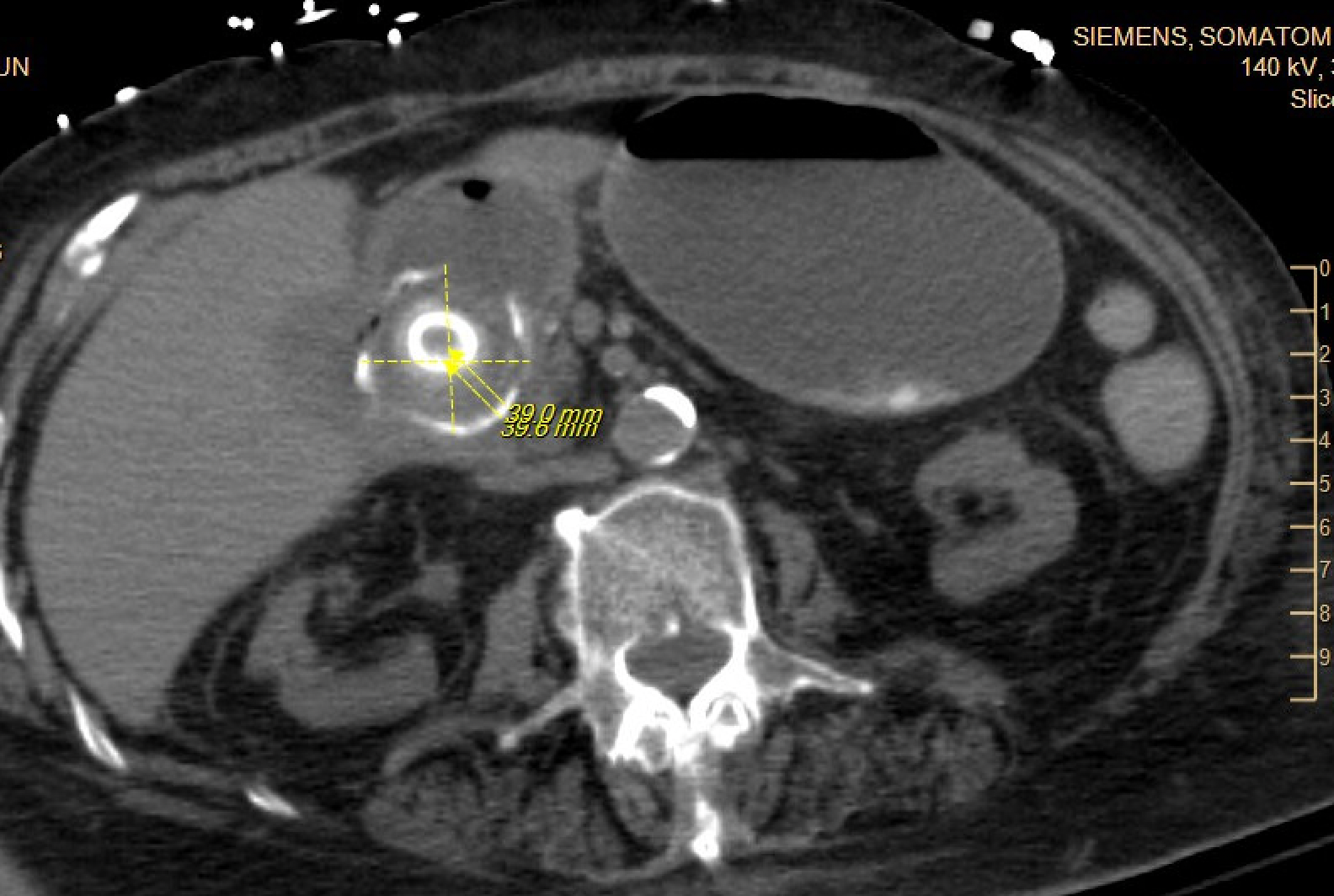
Case Presentation: An 84-year-old woman with type 2 diabetes mellitus, hypertension, prior ischemic stroke, osteoporosis, and rheumatoid arthritis presented to the hospital after a fall with altered mental status from increased home benzodiazepine use. During her admission, she developed acute nausea and vomiting with a new leukocytosis and was found to have acute cholecystitis. She underwent placement of a percutaneous cholecystostomy tube (PCT), completed intravenous antibiotics, and was discharged with the PCT in place. During her rehabilitation stay, her PCT was accidentally removed. She followed up with general surgery and was advised of the risk of gallstone complications, but given her frailty, the decision was made to allow for additional recovery prior to an elective cholecystectomy. Three months later, the patient presented to the emergency room with two days of abdominal pain, nausea, and vomiting. She had normal vital signs, and exam was notable for mild generalized abdominal tenderness, distention, and decreased bowel sounds. Laboratory evaluation revealed a white blood cell count of 21,100 cells/ul, a hemoglobin of 11.1 g/dL, normal sodium and chloride levels, a bicarbonate level of 36 mmol/L, blood urea nitrogen of 34 mg/dL, creatinine of 2.02 mg/dL (baseline is between 1.3 and 1.5 mg/dL). She had marked gaseous gastric distention on her initial abdominal x-ray. Subsequent computed tomography scan of the abdomen showed interval fistulization of the gallbladder and the gastric antrum/first portion of the duodenum with multiple gallstones extending through the fistula into the stomach and duodenum, resulting in gastric outlet obstruction, known as Bouveret syndrome. A nasogastric tube was placed for gastric decompression, and she underwent esophagogastroduodenoscopy for lithotripsy and removal of the gallstones. Attempted removal of the stones led to an esophageal tear. An esophageal stent was placed, but the patient developed bilateral empyemas requiring chest tube placement. She had a prolonged hospital course during which she was intubated and required enteral feedings through a nasojejunal tube.
Discussion: The prevalence of gallstone disease has increased over the last three decades and now afflicts about 14% of the population(1). Gallstones can lead to cholecystitis, choledocholithiasis, pancreatitis, Mirizzi syndrome, and gallstone ileus. This patient presented with Bouveret syndrome, a rare form of gallstone ileus in which a large gallstone migrates into the pylorus or duodenum via a cholecystoenteric fistula, causing gastric outlet obstruction(2,3). Management is challenging – both endoscopic approach with gallstone lithotripsy and surgical intervention have risk. Mortality is high, ranging from 12-30% due to the elderly age and comorbidities of those who develop Bouveret syndrome(3,4). Endoscopic intervention can lead to complications, including esophageal perforation as this patient experienced. With its nonspecific symptom presentation and significant mortality, Bouveret syndrome is a rare, but potentially lethal complication of gallstone disease.
Conclusions: Bouveret syndrome should be considered as a cause of gastric outlet obstruction in a patient with a history of gallstone disease. Prompt consultation from both gastroenterology and general surgery is essential to determining the most appropriate intervention in order to optimize outcomes.