Case Presentation: A 53-year-old male with a complex medical history including hypertension, diabetes, peripheral vascular disease, abdominal aortic aneurysm, and non-small cell lung cancer presented with persistent headaches, dizziness, and an unsteady gait. Initial CT scan revealed a left cerebellar mass with fourth ventricle effacement, prompting transfer to our intensive care unit for urgent neurosurgical evaluation. Admission labs and ECG were normal, and exam was significant for left-sided dysmetria. An MRI confirmed a 2 cm left cerebellar mass with edema consistent with metastatic disease. On hospital day 2, the patient was stable for transfer to the stepdown unit. During routine repeat head imaging, the patient suddenly collapsed and became unresponsive. Cardiopulmonary resuscitation and intubation were immediately initiated; initial cardiac rhythm was pulseless electrical activity (PEA) and patient required multiple shocks as per ACLS protocol. Pronouncement of death took place after a resuscitation effort totaling 27 minutes. Approximately five minutes later, the patient spontaneously resumed breathing with sinus rhythm on the cardiac monitor. The patient returned to the ICU without obvious neurological deficits. Subsequent cardiac workup showed no abnormalities, but the patient succumbed to postoperative complications on hospital day 16.
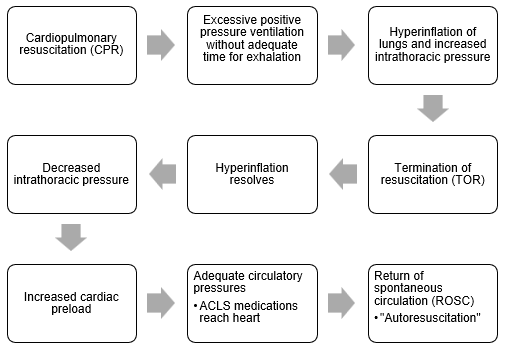
Discussion: Our case underscores a remarkable occurrence known as the “Lazarus phenomenon,” where a 53-year-old male experienced a return of spontaneous circulation (ROSC) five minutes after being declared dead. This phenomenon, colloquially named after the biblical figure who was revived by Jesus1, represents a rare event involving a revival after death. These occurrences are infrequently reported, with less than one-third of documented cases surviving2,4,5. The mechanisms of the Lazarus phenomenon are not entirely clear and involve many contributing factors such as reversible causes of cardiac arrest and duration of CPR6. The pathophysiology is thought to be related to excessive positive pressure ventilation leading to high intrathoracic pressure and the improved circulatory effects after termination of resuscitation (TOR)2. In this case, coronary ischemia was an unlikely reversible cause as it was a PEA arrest. Arrhythmia and electrolyte imbalances were considered but ruled out by ECG and laboratory studies. The presence of normal right ventricular systolic function on post-arrest echocardiogram also made massive pulmonary embolism an improbable cause. Another possibility, cerebellar tonsil herniation, ultimately led to the patient’s death two weeks following autoresuscitation. Some studies also suggest that the duration of the observation period upon TOR may influence the recognition of the Lazarus phenomenon2,3. One study found that no autoresuscitation was noted within a two-minute observation period, whereas some cases describe ROSC after at least a five-minute observation following TOR1,2,3.
Conclusions: The Lazarus phenomenon is rare and underreported. It emphasizes the need for avoiding excessive ventilation during CPR2 and continued monitoring following TOR. Awareness of this phenomenon during resuscitation efforts and its consideration in BLS/ACLS guidelines could potentially prevent false pronouncements and improve patient outcomes. Further research is warranted to better understand the duration of the observation period after TOR and the specifics of post-autoresuscitation care in the acute care setting.