
Background:
Non‐ST‐segment elevation acute coronary syndrome (NSTEACS) patients are managed either with a routine invasive strategy (RIS), in which all patients undergo coronary artery angiography, or with selective invasive strategy (SIS), in which only patients with refractory or inducible ischemia undergo coronary angiography. To evaluate whether the benefit of RIS or SIS is sex specific in NSTEACS patients, we performed a meta‐analysis of randomized clinical trials.
Methods:
PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials databases were searched up to September 2007. In addition, conference proceedings of the last 5 annual meetings of the American Heart Association, the American College of Cardiology, the European Society of Cardiology, and the Transcatheter Cardiovascular Therapeutics were manually searched. Clinical trials that randomized patients with NSTEACS to either RIS or SIS and reported death or nonfatal myocardial infarction (MI) outcomes separately for men and women were included. Data were abstracted independently by 2 investigators, and differences were resolved with mutual consensus. Results were pooled using a random‐effects model.
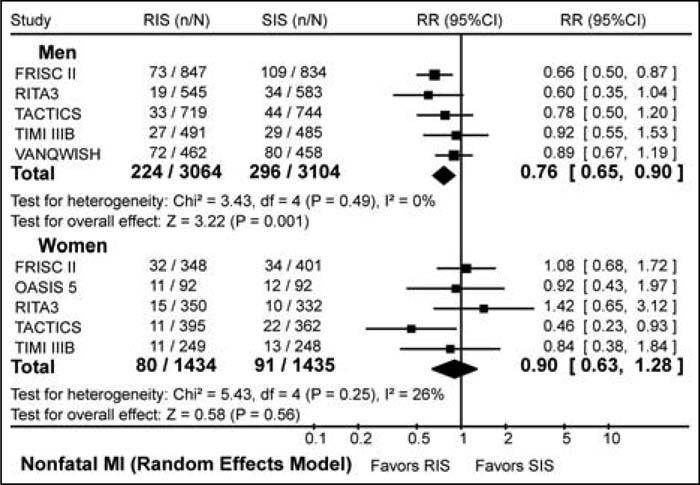
Figure 1. Forest plot of the nonfatal MI outcome in men and women for routine invasive strategy (RIS) and selective invasive strategy (SIS).
Results:
We identified 6 trials that included 6168 men and 2869 women. Men were younger than women (mean age 61 vs. 65 years). More men had a history of MI than did women (37% vs. 25%, respectively). Of the 3064 men randomized to RIS, 369 had composite outcome of death or nonfatal MI, whereas of the 3104 randomized to SIS, 436 had this outcome (RR = 0.84, 95% CI 0.65‐1.08). Of the 1434 women randomized to RIS, 132 had composite outcome of death or nonfatal MI, whereas of the 1435 randomized to SIS, 131 had this outcome (RR = 1.03, 95% CI 0.72‐1.45). In the RIS group, 151 men and 60 women died, whereas in the SIS group, 155 men and 47 women died (men: RR = 0.92, 95% CI 0.57‐1.48; women: RR = 1.28, 95% CI 0.732.25). Nonfatal MI occurred in 304 men and 80 women in the RIS group and in 387 men and 91 women in the SIS group (men: RR = 0.76, 95% CI 0.65‐0.90; women: RR = 0.90, 95% CI 0.63‐1.28). Thus, compared with SIS, RIS decreases the risk of nonfatal MI in men not women.
Conclusions:
Current evidence suggests that RIS is more effective than SIS in decreasing the risk of nonfatal MI in men but not in women. RIS does not appear to be better than SIS in reducing the risk of death in both sexes.
Author Disclosure:
R. Qayyum, none; J. Adomaityte, none; M. Navid, none; S. Nepal, none; M. Khalid, none.