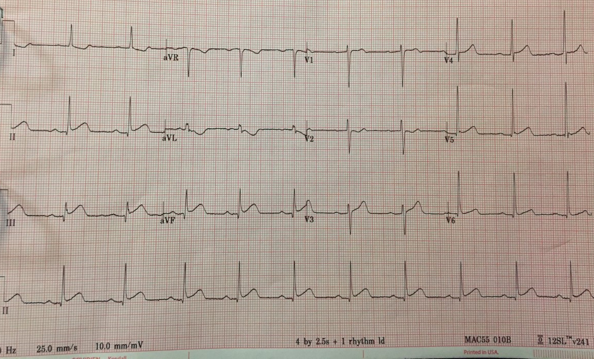
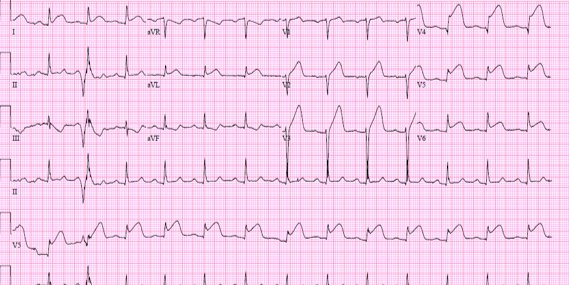
Case Presentation: A 35-year-old non-smoker male with a past medical history of hypertension presented to the hospital with worsening left-sided chest pain for 2 days. The chest pain was intermittent and associated with exertion. The patient denied any fever, cough or recent illnesses.On exam patient was slightly hypertensive with blood pressure 154/96, pulse rate of 62 and respiratory rate of 16. The cardiovascular exam was normal with no murmur or rubs appreciated. Lungs were clear to auscultation with no crackles, rhonchi or rales. Other physical examinations were unremarkable.Electrocardiogram was done in the emergency room which showed ST elevation in II, III and aVF with reciprocal ST depression in leads I and aVL(Fig.1). His lab was notable for mild leucocytosis of 12.8. Other labs were within normal limits. His initial Troponin I was <0.04ng/ml. Shortly after admission, he developed acute severe midsternal chest pain which was unrelieved with sublingual nitroglycerin. Repeat electrocardiogram showed significant precordial leads (V1-V6) and lateral ST elevation(I,aVL) with the resolution of ST elevation in inferior leads (Fig.2). The patient was emergently taken for cardiac catheterization and found to have ruptured plaque in the proximal segment with 80% stenosis and a wrapped around LAD. He underwent successful revascularization of the ruptured plaque with the placement of a drug-eluting stent. Follow-up echocardiogram showed severely decreased systolic function and an akinetic anterior septum, entire apex and severely hypokinetic mid lateral wall, basal inferior septum, and mid inferior wall.
Discussion: An electrocardiogram is an important diagnostic tool used to localize cardiac ischemia and infarction based on ST elevations. Wraparound LAD (Type III variant) supplies blood anteriorly and posterior inferiorly to the myocardium. Thus simultaneous ST-elevation could be observed in the anterior and inferior wall in wraparound LAD occlusion (1).In the presented case, the first electrocardiogram was consistent with inferior wall myocardial infarction. A second electrocardiogram done shortly after showed a change of ST elevation in precordial and lateral leads consistent with anterior myocardial infarction along with resolution of inferior wall ST elevation seen on the initial electrocardiogram. Given the change from inferior wall ST-elevation to anterior wall ST elevation, it is suggested that this is due to the force of the anterior wall injury creating reciprocal changes.In the literature simultaneous inferior and anterior ST elevation has been reported due to wraparound LAD. However, there has been only one case report to our knowledge that showed changes in electrocardiogram from inferior myocardial infarction to anterior myocardial infarction due to wraparound LAD occlusion(2).
Conclusions: Myocardial infarction results in necrosis of myocardial tissues due to coronary arteries occlusion. Acute occlusion of left anterior descending artery (LAD) usually results in ST-segment elevation in the precordial leads with reciprocal ST depression in inferior leads. This case details a rare presentation where the electrocardiogram changes from inferior myocardial ST elevation to anterior myocardial ST elevation infarction due to occlusion of wrap around LAD. It exemplifies the importance of serial electrocardiogram in the acute setting which can suggest wraparound LAD occlusion.