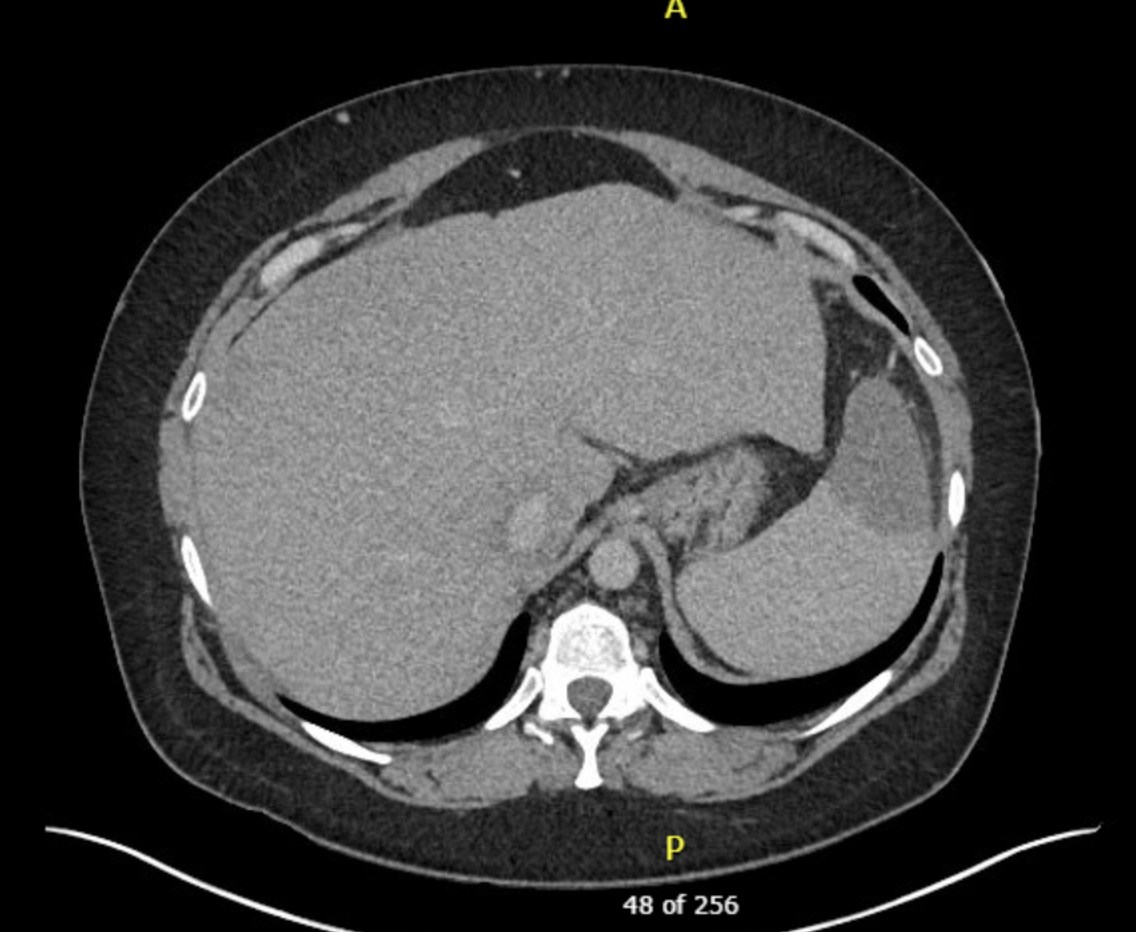
Case Presentation: A 46-year-old woman with alcohol use disorder, hypertension, and hepatic steatosis presented with 1 week of daily fevers and left upper quadrant abdominal pain. She reported chills, night sweats, cough, postprandial nausea and vomiting, and an intermittent unilateral headache but denied other focal symptoms, recent travel, or sick contacts. She was febrile to 103.1 degrees Fahrenheit, hypertensive, and tachycardic. Physical exam was notable for abdominal distension with left upper quadrant tenderness, hepatosplenomegaly, and bilateral lower extremity pitting edema. No scleral icterus, splinter hemorrhages, Osler nodes, lymphadenopathy, or rash was appreciated. Oropharyngeal exam was unremarkable. Initial labs revealed hyponatremia, acute on chronic transaminitis, elevated alkaline phosphatase, macrocytic anemia, thrombocytopenia, normal white blood cell count with bandemia, neutrophilia, lymphopenia, and elevated erythrocyte sedimentation rate and C-reactive protein. Respiratory pathogen panel and urinalysis were negative for infection. CT head was unremarkable. CT of the chest/abdomen was negative for pulmonary embolism but notable for an age-indeterminate splenic infarct with a wedge-shaped pattern and severe hepatosplenomegaly. Bilateral lower extremity ultrasound ruled out deep vein thrombosis. Transthoracic echocardiogram showed normal ventricular function and no vegetations. Blood cultures resulted negative. She continued to have headaches and nightly fevers to 103.2 degrees Fahrenheit. Hepatitis serologies were unrevealing. HIV, syphilis, TB, legionella, bartonella, brucella, Q fever, and fungal serologies were negative. Peripheral blood smear demonstrated polychromasia and anisocytosis with no evidence of a myelophthisic process. Antinuclear antibody was positive with a 1/80 titer. Her fever and lab abnormalities did not improve with an empiric trial of antibiotics nor prednisone. Monospot testing eventually resulted positive. Epstein-Barr Virus IgG, early antigen IgG, and nuclear antigen IgG were positive, but serum DNA was not detected. Cytomegalovirus (CMV) IgG was negative. CMV IgM was positive with markedly elevated DNA quantification. She was diagnosed with acute CMV infection and discharged with supportive care and resources for alcohol abstinence.
Discussion: CMV infection in an immunocompetent host is often asymptomatic but may present as a self-limited infectious mononucleosis-type syndrome characterized by fever, headache, malaise, and fatigue. Splenomegaly, cervical lymphadenopathy, and tonsillitis may also be seen. Diagnosis is typically via serology or molecular testing. Treatment is supportive; antiviral therapy is generally not indicated in immunocompetent hosts and symptoms tend to resolve in several weeks to months. However, CMV infection has also been associated with increased risk for venous thromboembolism in both immunocompetent and immunocompromised patients, with rare, life-threatening complications including pulmonary embolism and splenic infarct. This case illustrates that splenic infarct may be a presenting finding of acute CMV infection.
Conclusions: Fever with abdominal pain includes a wide differential diagnosis. While splenic infarct is a rare complication and not a pathognomonic finding associated with CMV infection, CMV should remain on the differential for immunocompetent patients presenting with fever of unknown etiology and splenic infarct.