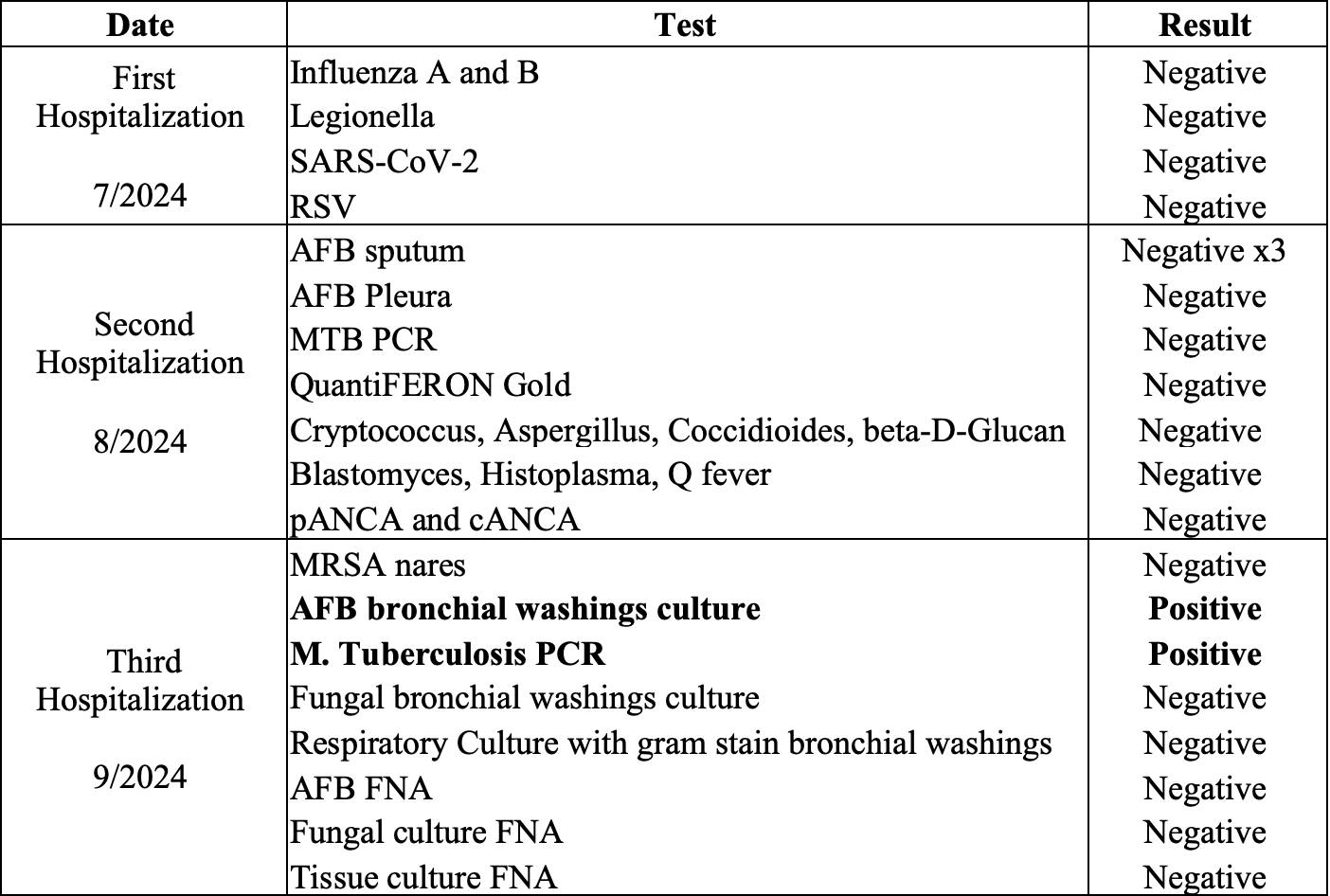
Case Presentation: A 76-year-old male with history of hypertension and recent travel to India presented to our health system with a history of sub acutely progressive dyspnea, low grade fevers, night sweats and chronic cough. Two months prior to this presentation, he was treated for community acquired pneumonia at an outside facility. About one month later, he presented to another hospital with persistent dyspnea and cough. Chest –Xray showed a large left pleural effusion. CT scan of the chest demonstrated centrilobular nodules with some tree in bud opacities and mediastinal lymphadenopathy. Peripheral serologic workup and pleural fluid analysis were negative for Tuberculosis (TB) (Table 1). He presented to our health system with persistent symptoms and bronchoscopy was performed. Bronchoalveolar lavage fluid was positive for Mycobacterium Tuberculosis by AFB staining and MTB PCR. He was started on Rifampin, Isoniazid, Pyrazinamide and Ethambutol and discharged with plan to follow-up with the Public Health TB control clinic.
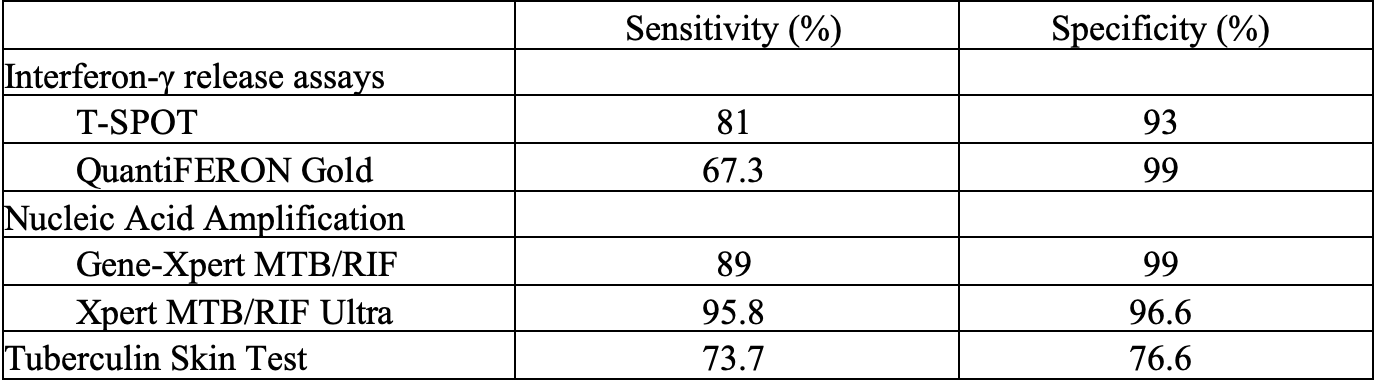
Discussion: This case demonstrates a three-month delay in the diagnosis of active TB and highlights the importance of maintaining a high index of suspicion in the context positive risk factors despite negative non-invasive diagnostic testing. Table 2 highlights the diagnostic accuracy of non-invasive TB testing. Bronchoscopic evaluation is indicated in specific circumstances including: 1) unsuccessful attempts to obtain sputum samples, 2) negative sputum studies in the setting of a high clinical suspicion of TB (as in this case), 3) suspected TB with drug resistance, and 4) when urgent diagnostic information is needed. Despite the wide availability of diagnostic tests, prompt diagnosis of TB remains challenging due to inconsistent sensitivity of AFB smears, prolonged culture times, and clinical mimicry by a variety of other diseases. These factors contribute to diagnostic delay as demonstrated in this case where TB was misdiagnosed as community acquired pneumonia, preliminary testing was negative, and bronchoscopy was not performed until three months after initial presentation. Missed or delayed diagnosis of TB can be catastrophic because it affects patients and community through delayed treatment, increased period of infectivity, increased transmission of disease, and increased medical costs and mortality. Strategies for hospitalists to avoid cognitive errors include, paying attention to disease timeline, focus on diagnostic accuracy rather than just symptomatology, understanding pre-test probability of an illness based on prevalence, and continual consideration of other diagnoses when a patient’s symptoms do not improve with treatment.
Conclusions: Hospitalists should be aware of the limitations of TB testing and maintain a high index of suspicion despite negative diagnostic testing. Also, recognizing contributing factors to cognitive errors is a critical skill for hospitalists to provide high-value and cost-effective care for patients.