Case Presentation: 52-year-old male presented with six-week history of unintentional weight loss, decreased appetite and non-radiating dull suprapubic pain. Review of systems was notable for constipation, polyuria, polydipsia, nausea, and left leg swelling. No family history of cancer or blood dyscrasias. Physical examination revealed blood pressure- 194/114 mmHg, heart rate -105, distended abdomen with hypoactive bowel sounds, diffuse erythematous rash on left lower extremity.
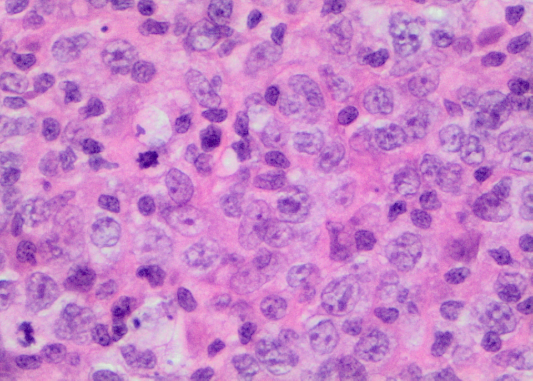
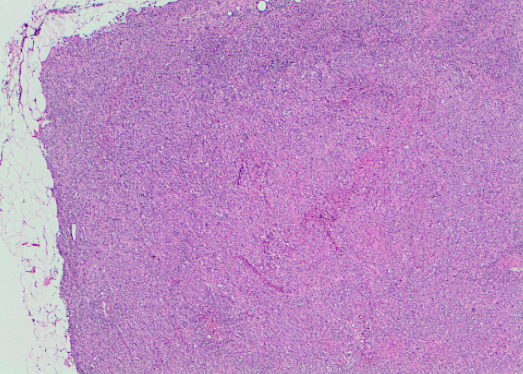
Labs showed hypercalcemia- 15.6 mg/dl, creatinine- 2.43 mg/dl, 25-OH vitamin D- 14 ng/ml, 1,25 dihydroxy vitamin D- 113 pg/ml, PTH- <7 pg/ml and PTHrP- 18 pg/ml. Serum and urine electrophoresis were unremarkable. Chest/abdominal/pelvis CT without contrast showed extensive retroperitoneal and pelvic lymphadenopathy. Lymph node biopsy showed diffuse large B-cell lymphoma, germinal center type.
He initially received IV Lasix, one-time IM Calcitonin, and normal saline boluses after which normal saline at 200 ml/hour, daily intramuscular Calcitonin for two days, and one-time IV Pamidronate was given. Calcium level decreased from 15.6 mg/dl to 11.6 mg/dl but later increased to 13.3 mg/dl, thus second dose of IV Pamidronate and IV Lasix was given. Repeat calcium was 12.1 mg/dl prompting treatment with Prednisone 30 mg daily, this led to gradual but sustained improvement in calcium level. Creatinine trended downwards and patient diuresed appropriately.
Discussion: Hypercalcemia is a common endocrine problem caused by primary hyperparathyroidism and malignancy in 90% of cases. We present a diffuse large B-cell Lymphoma patient case with 1α,25-(OH)2D3-mediated hypercalcemia.
Common mechanisms described in malignancy-related hypercalcemia include production of PTHrP, osteolytic metastases and excessive calcium release from bone. 1,25 dihydroxy vitamin D level is suppressed in these mechanisms. Excessive production of 1,25 dihydroxy vitamin D accounts for 8% of diffuse large B cell lymphoma cases.5 In calcium metabolism, PTH activates 1-alpha-hydroxylase enzyme in renal proximal tubules which converts 25-hydroxyvitamin D to more active 1,25-dihydroxyvitamin D. Mechanism of 1,25 dihydroxy vitamin D-mediated hypercalcemia remains unclear.
Management of hypercalcemia is based on symptoms and severity. Hypercalcemia of malignancy is an oncologic emergency. Treatment is indicated when calcium exceeds 14mg/dl or in symptomatic patients. Hypercalcemia causes dehydration from nausea and vomiting, hypercalcemia-induced nephrogenic diabetes insipidus; adequate hydration with IV fluids is important. 9 Calcitonin is an important adjunct medication.10 Bisphosphonates are used in treatment of hypercalcemia of malignancy. IV hydrocortisone and oral prednisone are treatments of choice in 1α,25-(OH)2D3 mediated hypercalcemia because steroids inhibit calcidiol into calcitriol, decreasing intestinal calcium absorption.
Conclusions: Hypercalcemia mediated by calcitriol is rare. Few case reports document this occurrence in sarcoidosis, hematologic malignancies or mycobacterium infections. Calcitriol-mediated hypercalcemia accounts for less than 1% of all malignancy-related hypercalcemia; and is primarily associated with Hodgkin lymphoma. Our patient has diffuse large B-cell Lymphoma as the etiology of hypercalcemia.