Background: Hospital-at-Home (HaH) is a novel care model providing inpatient care for patients in their home through a combination of home visits and virtual care. Advanced Care at Home (ACH), UNC Health’s HaH program, launched in 2021, has helped over 2,000 admissions to date. The majority of HaH care is provided under the terms of the CMS Acute Hospital Care at Home (AHCAH) waiver issued in November 2020. This waiver removes the Medicare hospital condition of participation that requires 24/7 onsite nursing; however, acquiring patients is a complex, labor intensive processes involving manual chart review, screening, and ACH admission. This provides a challenge to the growth and stability of the program.
Purpose: We created an optimized standard procedure for ACH patient acquisition through work lists aligned with the acquisition funnel, then tasking eligible patients through the lists. Our goal was to ensure the financial security of ACH by increasing our Average Daily Census (ADC).
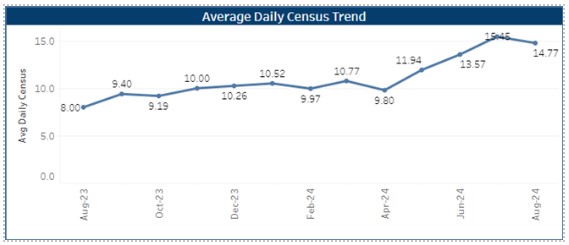
Description: Previously, our acquisition workflow involved shared responsibilities across the three-provider team, the nurse Patient Admissions Officers (PAO), and the clinical manager of ACH. Patients were filtered onto eight triage lists (Figure 1) by eligible payor and residence within an eligible zip code for our catchment area. Initial reviews were coded in a free-text box as: Early Emergency (ED), Evaluation, Contact, or Accepted. If a patient was appropriate, the acquiring provider would send a chat through our electronic health record (EHR) system to the inpatient attending for approval before performing a social screening checklist. If accepted, the ACH provider team was alerted, and transportation was coordinated to bring the patient home. When this information was communicated in a free-text box, there was no sorting or shared awareness of the patient’s status in the acquisition process. This led to a lack of clear task ownership, duplicative reviews, and no process to follow patients who were either too acute or at observation status at initial review. Members of the ACH leadership team and PAOs met with an EHR analyst to create a new workflow addressing these challenges. We split the acquisition process into three stages: Initial Triage, Needs Clinical Review, and Needs Social Stability Review. The triage lists remains the same, and a new “Under Consideration” status was created for patients who required follow up to pass their clinical screen or their social stability screen. If these screens are passed, the patient is accepted to the program and transport is scheduled (Figure 2). These are discrete EHR flowsheet fields. This creates greater insight into team workflow and quantity of screening touches required, as well as specific follow updates. Since the introduction of these workflows in July 2024, we have had consecutive months of census growth (ADC 11.2 from Jan-June 2024, then ADC 15.11 for July and August).
Conclusions: This new workflow improved the acquisition of patients for a HaH program based at an academic medical center and community hospital. By creating a more standardized workflow, our program acquired and cared for more patients, contributing to the financial stability of the program.