Background: Effective communication between the inpatient care team, patients and their families is an integral part of high quality, safe care while inpatient and during transitions of care. Collaborative, highly functioning interdisciplinary teams can impact the perception of that care by the patient and family. A multidisciplinary team at Utah Valley Hospital piloted an accountable care unit (ACU) in August of 2022 on a medical surgical floor with a 2-prong approach: hospitalist geographic cohorting paired with a highly efficient interdisciplinary daily huddle. The team included nursing, hospitalist physicians, case managers, occupational and physical therapists, pharmacists and hospitalist coordinators (a role unique to Intermountain Health in which an RN rounds in tandem with the hospitalist provider to ensure safe and efficient transitions of care). The intent of this pilot was to implement an interdisciplinary rounding model with the goal of improving both patient and care team satisfaction as well as care team efficiency. We sought to improve upon metrics such as length of stay (LOS) and likelihood to recommend (LTR).
Methods: Patients on a 36-bed medical surgical unit were distributed between two hospitalist physicians daily. An interdisciplinary daily huddle replaced the existing discharge planning meeting. In the huddle, each patient was reviewed in a structured, comprehensive fashion with all disciplines providing input to assess additional needs or interventions to progress the plan of care. In conjunction with this structured review, patients were rounded on in a dyad fashion, meaning the provider, hospitalist coordinator and bedside nurse round together at the bedside using a structured communication report/agenda. The KATA continuous improvement tool was utilized to progress 7 iterations of the model in a stepwise fashion over a total of 7 months. No other significant, concurrent changes were implemented on the unit over the course of the pilot.
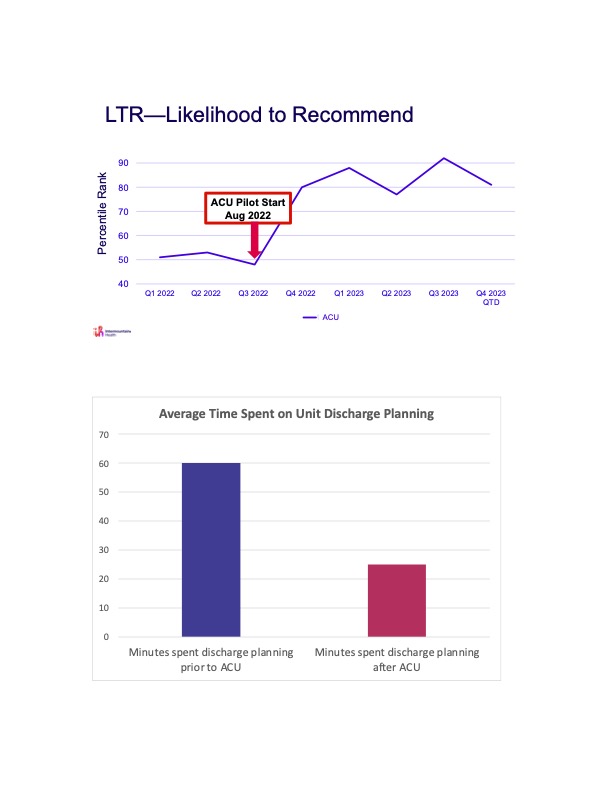
Results: LTR improved from 61st percentile rank to 91st percentile rank and patient perception of physician communication improved from 2nd percentile rank to 90th percentile rank. We saw a significant reduction in LOS by 12 hours. These metrics were measured quarterly. Discharge planning efficiency for all patients on the unit improved from 60 minutes to 25 minutes per day.
Conclusions: The implementation of an interdisciplinary collaboration rounding model led to improved efficiency metrics, such as LOS, and patient experience metrics, such as LTR. As a result of the dramatic improvement in these metrics, there is excitement to scale the ACU model throughout all medical surgical units at Utah Valley Hospital. Necessary steps include a transition to geographic rounding, requiring coordination with nursing supervisors, other service lines and hospital administration. Barriers to this are difficulty with throughput within a busy hospital system and unequal census between providers. Hospitalist group buy-in to this model will be pivotal to successful implementation on all medical surgical units. Intermountain Health’s commitment to hospitalist coordinators is a strategy which will help provider acceptance of this new model given their impact on team efficiency during high census days. Moving forward, the impact of this model on provider satisfaction will be studied.