Case Presentation:
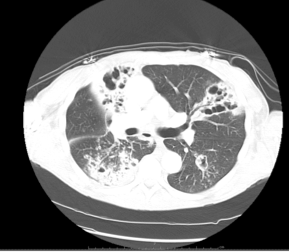
53-yo Male with past medical history of poly-substance abuse presented with weakness, shortness of breath and productive cough for 1 month. He also reported low-grade fever, chills, fatigue, and weight loss of 30 to 40 pounds. He had 25-pack-year history of smoking. On examination, he had bronchial breath sounds in right upper lung zone. Chest X-ray showed extensive consolidative infiltrate in the right upper lobe with areas of cavitation and volume loss. (Figure 1) CT scan of chest revealed large consolidation with volume loss and cystic changes in the right upper lobe. consistent with mycobacterial infection. (Figure 2) Acid-fast bacilli staining and later on culture were positive for Mycobacterium tuberculosis. He was started on anti-TB medications. Patient developed altered mental status 3 weeks after presentation which was associated with concomitant rapid rise in calcium levels. 25 Hydroxy- Vitamin D was found to be low (27 pg/ml); whereas 1,25 Dihydroxy Vitamin D was in high normal range (48 pg/ml). PTH related Protein (PTHrP), and PTH levels were normal. Full body bone scan and multiple myeloma was negative. 24 hour urinary calcium was elevated at 562 mg. Patient was given aggressive hydration and later on steroids for hypercalcemia. He showed marked improvement in his mental status with correction of his hypercalcemia within a week after steroids were introduced.
Discussion:
Hypercalcemia is known to occur in granulomatous diseases and although infrequent is a well recognized complication of active tuberculosis (TB). Activated macrophages in granulomas possess 1-a hydroxylase which converts 25-hydroxyvitamin D to its active form 1-25-hydroxyvitamin D. PTHrP, the usual etiologic agent of humoral hypercalcemia of malignancy, has been shown to be elevated in patients with other granulomatous diseases like sarcoidosis and may also contribute to the hypercalcemia in some patients with tuberculosis. We report a challenging case of acute encephalopathy caused by hypercalcemia secondary to active pulmonary tuberculosis and its medical management and outcome.
Conclusions:
Hypercalcemia is reported in 16% of the patients with TB in United States. Out of the patients who are hypercalcemic only 12% develop symptoms. Hypercalciuria due to hyperabsorption of dietary calcium is more common than overt hypercalcemia Increased intestinal calcium absorption induced by high serum calcitriol concentrations is the primary abnormality. Our patient had low 25- hydroxy Vitamin D levels but high normal 1,25 Dihydroxy Vitamin D along with hypercalciuria. Hypercalcemia, as a manifestation of sarcoidosis, frequently resolves with glucocorticoids, but to our knowledge, this is only the fourth reported case of treatment of hypercalcemia in TB with steroids.