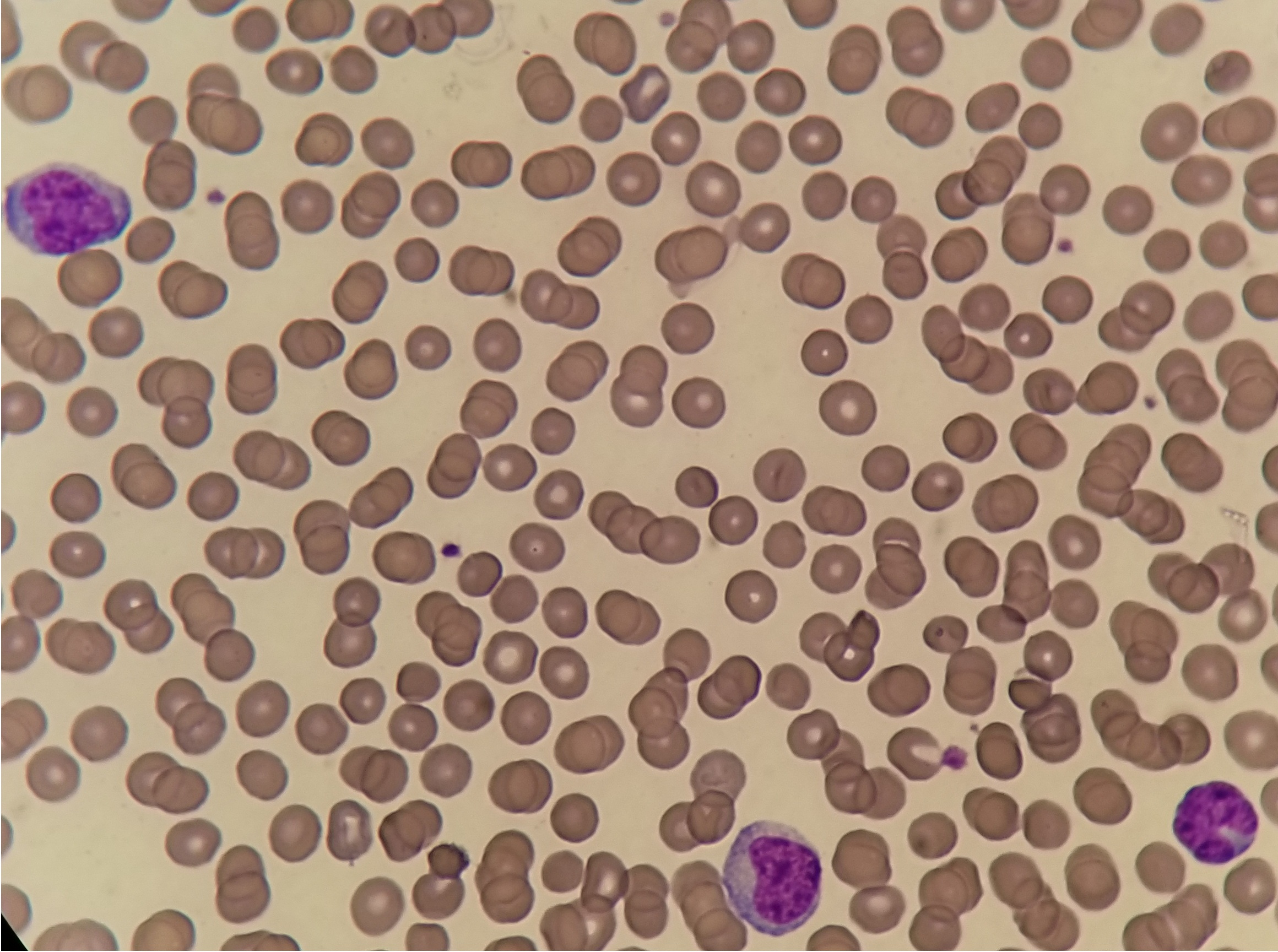
Case Presentation: A 29-year-old woman presented to the emergency department for a 5-day history of persistent fever, sore throat, diffuse myalgias, and epigastric abdominal pain. The patient was recently diagnosed and treated for pelvic inflammatory disease after unprotected intercourse with a new sexual partner. On examination, she was tachycardic, hypotensive, afebrile and was noted to have scleral icterus and mild hepatosplenomegaly. Lab studies revealed a WBC 5.0 ^3/µL with 32% blasts, platelets of 94K. Further lab testing revealed a mixed hyperbilirubinemia with T.bili 4.1, ALT 521 U/L, AST 424 U/L, Alk Phos 210 U/L. HIV Ag/Ab and HCV RNA were negative. The abdominal US confirmed hepatosplenomegaly without biliary abnormality. Peripheral smear displayed atypical lymphocytes and blast cells, no Auer rods were seen. Hematology was consulted for possible acute leukemia, and promptly recommended flow cytometry and consideration of bone marrow biopsy. Flow cytometry revealed slightly abnormal antigen expression in granulocytes without an increase in blasts and no evidence of a B-cell or T-cell lymphoproliferative disorder. A Monospot was eventually obtained and was positive, consistent with EBV Infectious Mononucleosis. Bone marrow biopsy was deferred and the blasts, thrombocytopenia, and hyperbilirubinemia with transaminitis were attributed to Infectious Mononucleosis. The patient was discharged from the hospital with routine outpatient follow-up.
Discussion: Epstein-Barr virus (EBV) is a herpesvirus that primarily infects B cells and typically becomes latent in the human B lymphocytes for their entire lifetime. In immunocompetent hosts, humoral and cellular immunity usually controls the primary infection without incident. Occasionally, this condition advances into infectious mononucleosis and can resemble or cause acute leukemia, lymphoma, and many other hematologic emergencies. EBV pathogenesis to lymphoma and leukemia has been attributed to its chronic active phase that stimulates cellular proliferation and increases the risk of pathologic transformation.
Conclusions: EBV infection is a self-limited infection that primarily infects B cells. It can transform B cells into proliferating blasts, mimicking acute leukemia and other lymphoproliferative disorders. A multidisciplinary team and broad differential are critical to providing timely, comprehensive care to patients that present with these concerning clinical features.