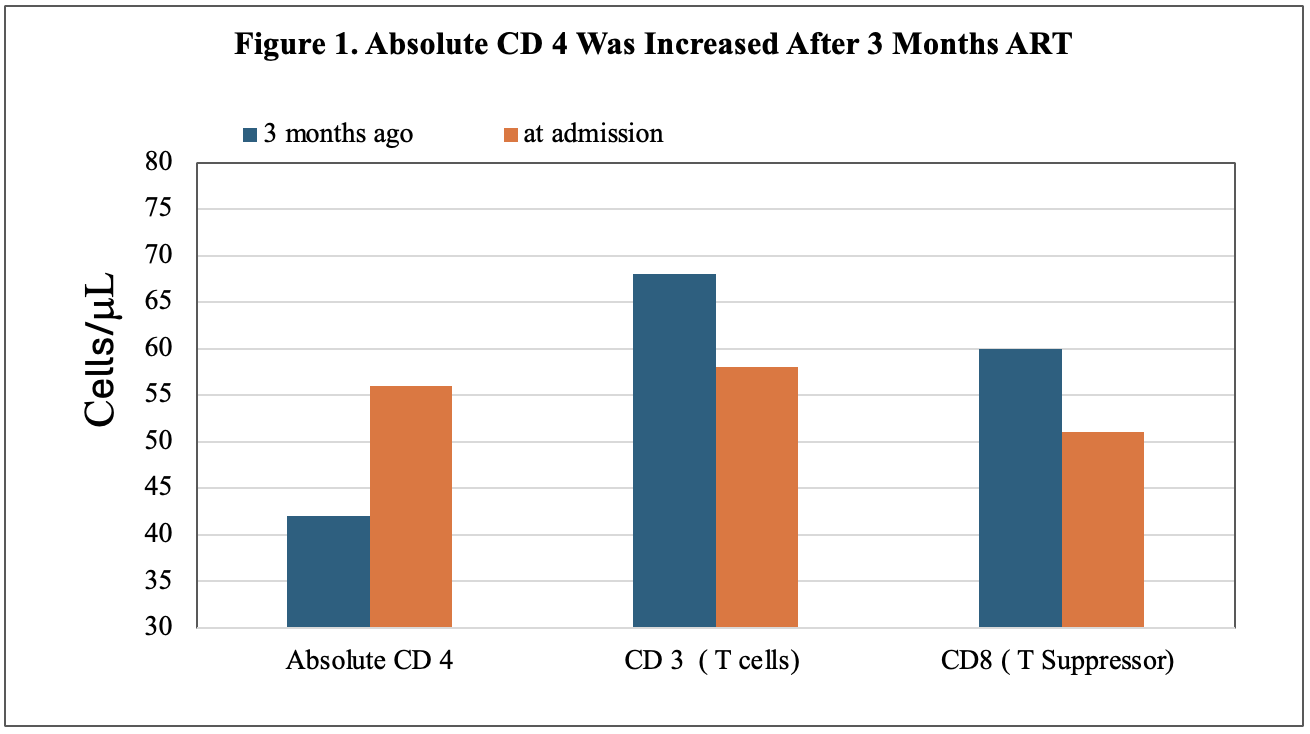
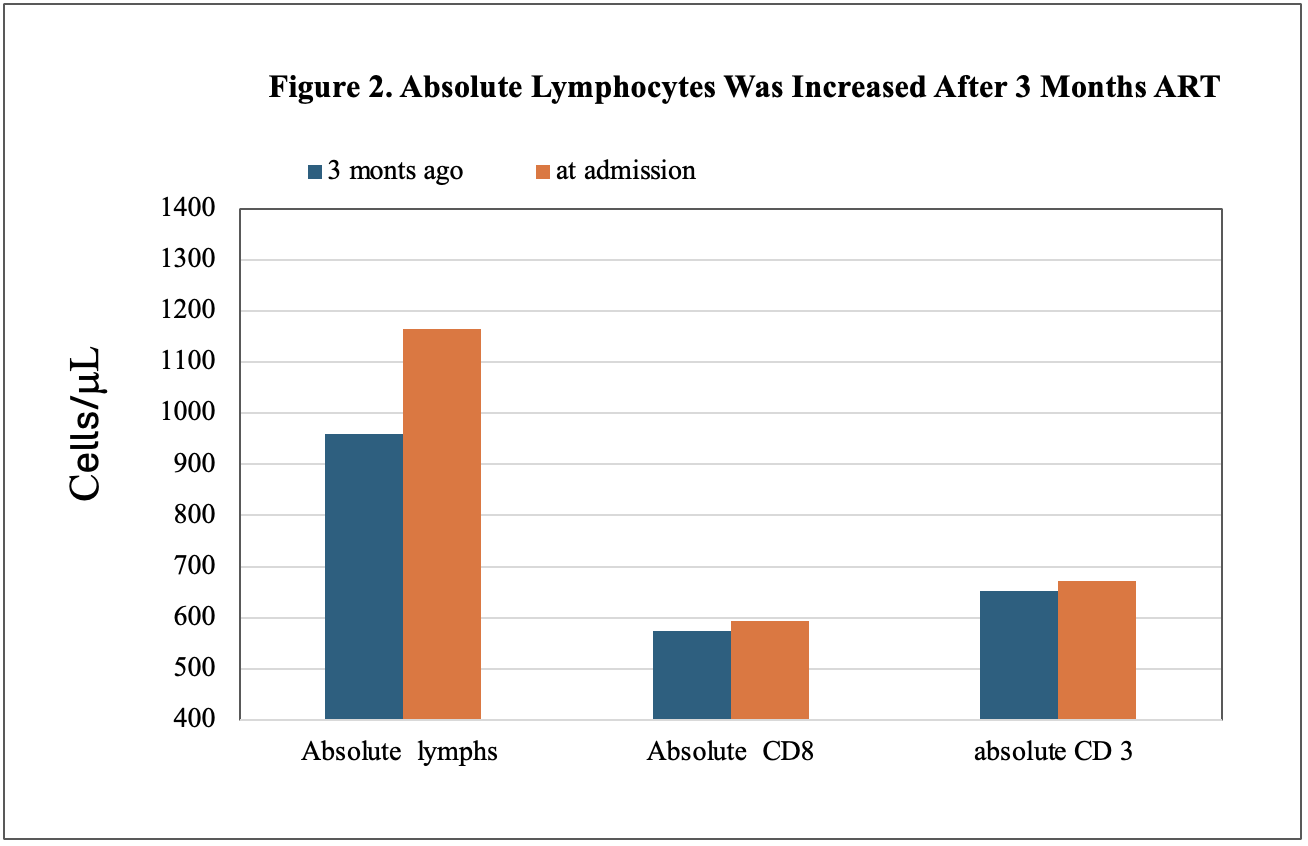
Case Presentation: 39-year-old man with PMH of HIV presents to the ER with chief complaints of progressive headaches for 4 days associated with projectile vomiting about 50 times/day. The patient reported that he has not taken anti-HIV medication for a few years, he started to take Biktarvy (bictegravir, emtricitabine, and tenofovir alafenamide) 3 months ago and has not missed a dose. Physical Examination, unremarkable, no focal neurologic deficits. Laboratory tests: WBC: 11.87K. CT of the head showed no acute abnormality; all other tests were unremarkable. The patient initially was treated with IV ceftriaxone, acyclovir, dexamethasone, and vancomycin. After admission, infectious disease and neurology were consulted; serum cryptococcal antigen was 1: 647. Lumbar puncture (LP) was performed, CSF Cryptococcal antigen was positive, CSF aerobic culture and PCR were positive for Cryptococcal, analysis of cerebrospinal fluid (CSF) showed protein was 59 mg/dl, Glucose was 67 mg/dl, differential of CSF with 98% of lymphocytes and 2% of monocytes. The patient received IV amphotericin B and oral therapy (PO) flucytosine 500 mg q6h for 5 out of 14 days. The patient’s symptoms were gradually improving; oral fluconazole was prescribed after discharge, and the patient was advised to follow up with ID consult and to repeat the LP. CD4 T-cell count & flow cytometry were performed at admission, compared with restarted anti-HIV therapy 3 months ago (Figure 1). At admission, absolute lymphocytes and CD4 were increased (Figures 1 and 2), and HIV RNA was not detected, which was 40900 copies/ml 3 months ago.
Discussion: Cryptococcal meningitis (CM) is a leading cause of death for human immunodeficiency virus (HIV) patients. Extraordinary CM is associated with immune reconstitution inflammatory syndrome (IRIS), presents as clinical worsening or new presentation as an “unmasking” of previously unknown cryptococcal disease after beginning antiretroviral therapy (ART), with a reduction in peripheral blood HIV viral load and the initiation of CD4+ T cell recovery. Non-compliance with ART is a major barrier to successful treatment for HIV-infected individuals. After starting ART therapy, a rising CD 4 count is a primary goal of treatment; however, there is also a potential for IRIS due to an overreaction to other infections that were already present or possible infections that were already present in the body. An IRIS mostly occurs in the first 4 months after ART therapy, especially in the presence of mycobacterial, chronic viral, protozoan, or fungal infections, but the detailed immune mechanisms remain unclear. Cryptococcal Meningitis IRIS (CM-IRIS) remains with an average mortality rate of around 20%. There are two clinic types of IRIS, paradoxical refers to the recurrence of clinical signs of a previously treated opportunistic infection, and unmasking type, when a patient with HIV experiences a new infection or the uncovering of a previously undiagnosed and asymptomatic infection shortly after starting ART as our case’s presentation
Conclusions: This case report highlights the importance of recognizing that Acute Unmasking CM-IRIS after ART therapy occurred in a patient with a history of non-compliance with ART, the severity and extent of which have been less frequently reported. An accurate review of past medication history at admission is critical to detect anti-HIV drug-related pathology and minimize the risk of non-compliance with ART medication.