Background: The Reducing REVISITS study enrolled and randomized diverse hospitals to identify scalable solutions for reducing preventable acute care for patients with chronic obstructive pulmonary disease (COPD) utilizing Society of Hospital Medicine’s (SHM’s) award-winning mentored implementation model (MIM). MIM provides one year of expert advice and tools through virtual site visits and monthly meetings to review program implementation progress and data and strategies for bypassing practice-change impediments. We adapted the MIM to include virtual components (e.g., training, site visits); half of sites also received codesign support. We paired trained physician mentors who with quality improvement (QI) expertise with site leads to guide implementation of COPD transition of care (ToC) bundles implemented virtually or in-person.
Methods: Physician mentors (n=12) were trained in QI skills, study methods, and COPD ToC interventions (e.g., medication reconciliation, inhaler education, etc). Mentors received at least 7 hours of training, over 3 virtual sessions (July 2022 – January 2023) including didactic sessions, rationale for change in care for COPD inpatients, discussing case-based scenarios, and employing best MIM practices. Post-training SHM provided resources to guide monthly mentor calls with sites and facilitated monthly mentor-specific calls to provide ongoing support to all mentors. Mentors (n=12) and site leads (n=43) completed quarterly MIM evaluations during the implementation period. (Table 2)
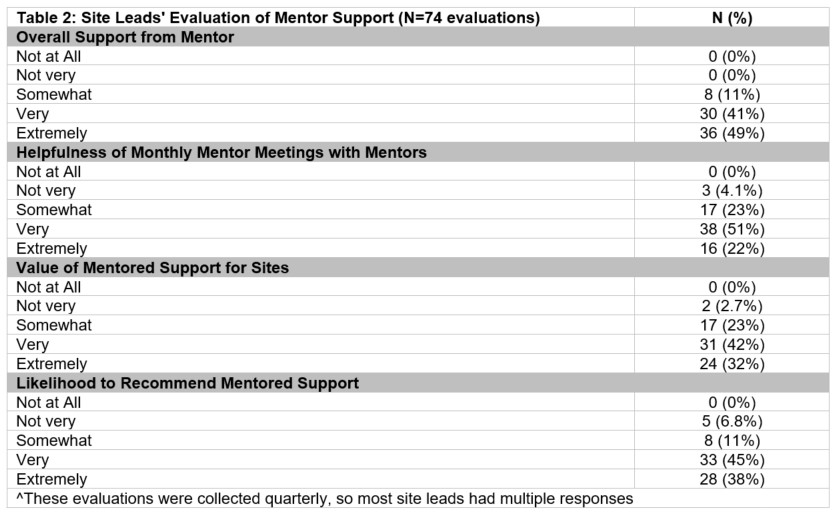
Results: The majority (83%) of mentors rated the overall training and all three training sessions [orientation session (83%) and the initial (75%) and follow-up (83%) ‘mentor university’ trainings] as very or extremely helpful. After training, all (100%) mentors reported that they were somewhat (50%) or very (50%) confident that the training adequately prepared them to mentor sites. Most reported having at least some general ToC (100%), COPD-specific ToC (92%), and/or general QI (100%) expertise to inform their mentoring sessions. The majority (98%) of mentors reported feeling prepared for their virtual monthly mentoring meetings with assigned sites and almost all (96%) indicated they felt meetings were at least somewhat impactful to site leads. [Table 1] In turn, most site lead evaluations indicated that they were at least somewhat supported by their mentor (100%), found the mentoring helpful (96%), and found value in the mentored support (97%). Notably, 83% of site lead evaluations reported being very or extremely likely to recommend mentored support to peers, further highlighting the perceived effectiveness and value of the program. [Table 2]
Conclusions: The MIM is an innovative framework for implementing QI programs to improve care for patients as they for transition from hospital to home. Effective training and guidance of mentors is essential for optimizing successful program implementation. Evaluation data from mentors underscore the value of training for adequate mentoring preparation with site leads benefiting to support improved COPD ToC care delivery. Site leads report being supported and helped by their mentors. In this study, we demonstrated the MIM can be successfully adapted by incorporating robust, virtual training and MIM monthly meetings to translate effective mentoring strategies into practice to fulfill the objective of improving ToC for patients with chronic conditions such as COPD.